Soft sonor [L'] appears in a child’s speech in the second or third year of life, hard [L] - at 5-6 years, which is associated with more complex articulation, requiring strong muscles of the tip of the tongue and its upper rise. In the absence or distorted pronunciation of a phoneme, lambdacism is diagnosed; when it is replaced with other speech sounds, paralambdacism is diagnosed. Along with sigmatisms and rhotacisms, pronunciation defects [L-L'] are among the most common sound distortions among preschool children with speech disorders (from 10% with dyslalia to 46.7% with erased dysarthria).
Causes of lambdacism
Deficiencies in pronunciation [L-L'] are typical for children suffering from functional and mechanical dyslalia, dysarthric disorders, and open rhinolalia. Organic defects in the peripheral speech organs, impaired muscle innervation, and functional insufficiency of sound pronunciation can lead to lambdacism:
- Shortened hypoglossal ligament.
It does not allow the upward movement of the tongue, which is necessary for the formation of the desired articulatory pattern. As a result, the child finds an available compensatory position (interdental, labiodental, etc.), which replaces correct articulation. - Macroglossia and microglossia.
If the language is underdeveloped, it becomes impossible or difficult to pronounce all linguistic phonemes, including dental [L-L']. The small size of the organ makes it impossible for the tongue to approach the upper incisors. With a massive tongue, both its upper rise and narrowing of the tip are difficult. - Changes in muscle tone.
With dysarthria, the tongue may be flaccid, paretic or tense and spastic. These factors significantly distort articulation. The tone of the orbicularis oris muscle is also impaired, which is accompanied by difficulties in voluntarily opening and holding the lips. - Palatal clefts.
Compensatory features for rhinolalia are a high elevation of the root of the tongue, a shift of articulation into the depths of the oral cavity, and non-participation of the tip of the tongue in the formation of sounds. [L] is usually absent or appears bilabial. - Hearing loss.
Hearing loss can be accompanied by both mixing and substitution of sound due to impaired acoustic differentiation, and distorted pronunciation due to inaccuracy and blurred articulation. - Other reasons.
Lambdacism can be caused by the lack of formation of correct speech kinesthesia as a result of speech deprivation and sickness in children. Another reason is copying incorrect sound pronunciation, including dialectal features in a bilingual environment.
Reasons for incorrect pronunciation of “L”
There are no unexplained causes of speech impediment. Doctors identify only three main conditions under which children cannot pronounce “l” correctly:
1. In speech, the child does not perceive “L” phonemically.
Phonemic hearing is what allows a person to distinguish one speech sound from another, hear words correctly and understand them well. Doctors recommend developing this hearing in babies from birth. That is, you need to talk to children without distorting words, so that they hear what will later be used in everyday speech. It must be remembered that written language is also formed on the basis of oral speech. Phonetic awareness thus influences future reading and writing skills. Normally, by the age of 4, a child should confidently distinguish one sound from another and not confuse “night” with “daughter” and “bear” with “mouse.”
2. The second reason for the incorrect pronunciation of “l” is the short hypoglossal ligament, due to the anatomical structure.
3. The inability to say “l” can also be a consequence of weak muscle tissues of the tongue.
We should not forget that for two- to three-year-old children, errors in speech starting with “l” are considered the norm. The formation of the correct pronunciation of “L” refers to older ages - 4 and even 6 years.
Phonetic characteristics of the sounds [L] and [L']
The sound [L] is a consonant, transitive, oral, anterior lingual. When it is articulated, the lips assume a half-smile position and the teeth open. The tongue is saddle-shaped, with a narrow tip resting on the base of the upper incisors. The edges of the tongue form a gap with the lateral teeth through which air escapes. The vocal folds are brought together and vibrate to form the voice. This is the only phoneme in the Russian language that is pronounced in a narrow language.
When pronouncing [L'], the tip of the tongue is raised towards the alveoli and is more tense. The anterior-middle sections of the back of the tongue are close to the palate, giving softening (palatalization).
Position of the tongue when pronouncing the sound [L]
Preliminary articulation exercises
Before moving directly to exercises for making the sound “l”, experts advise doing a series of articulation tasks, the so-called articulatory gymnastics, which precedes the approach to making the sound “l”. This is a kind of tuning of the speech apparatus to master the rebellious sound. Here we work on the movements of the lips and tongue.
To begin with, the child is told and shown the structure of the mouth: lips, upper and lower; behind them are the teeth, upper and lower; at the top - a tubercle; behind it is the hard palate, it continues with the soft palate and ends with the velum palatine, on which there is a uvula. If a child is diagnosed with lambdacism in any form, then first you need to do the following articulation exercises (perform every day in front of the mirror, counting from one to five, for five to ten minutes, twice a day):
- “Smile” - part your lips into a smile, exposing your upper and lower teeth.
- “Tube” - lips are closed and extended forward.
- “Tongue punishment” - the tongue remains on the lower lip, it is spanked, saying “Pa-pa-pa.”
- “Cleaning the upper teeth” (from the inside) - the tongue is made wide, it is moved from side to side at the upper tubercles, also known as alveoli.
- “Sail” - the tip of the tongue should be rested on the row of upper front teeth. The tongue is like a hammock that has sagged. There is no need to move the tongue, it is simply held in this position while counting. The longer you can hold on, the better.
- “The cat drinks milk” - a wide tongue licks the upper lip from top to bottom.
- “Turkey chatter” is the same as in the “cat” exercise, but the movements are fast and accompanied by the sounds “bl-bl-bl-...”.
- “Swing” - with your mouth slightly open, you need to smile widely. On the count of “1-2”, the tip of the tongue rests on the upper and then on the lower incisors (from their inner side).
- “Horse” - click the wide tip of the tongue on the palate behind the upper front incisors. The mouth is open, but the lower jaw does not move at all.
- “Fungus” - the tongue seems to be glued to the palate, the hyoid frenulum is tense.
It is recommended to carry out such gymnastics for two to four weeks. In this way, the skill is developed to fix the necessary articulatory posture, accurately make all movements and monitor the lips, tongue and the entire speech apparatus.
Types of lambdacism
The hard [L] is the most complex articulatory, therefore it is violated much more often than its soft pair. The following types of lambdacism are described in speech therapy:
- Bilabial (labial-labial).
The most common phonetic defect. The tongue is not involved in articulation; the sound is formed by bringing the lips together, resulting in something similar to English [W]. - Labial-dental.
The lower lip comes closer to the upper teeth, as a result of which a sound similar to [B] is heard. - Interdental.
The tip of the tongue is inserted between the lower and upper incisors, but the interdental [L] does not differ by ear from the correctly articulated one. - Nasal.
The back of the back of the tongue closes with the soft palate, while the air exits through the nasal cavity, making the sound reminiscent of [N] or the combination “NG”. - Side.
Pronunciation is accompanied by swelling of the cheeks (sometimes on one side) and additional noisy sounds. Often combined with lateral rhotacism and sigmatism of sibilants. - Softened.
Instead of a hard phoneme, its semi-softened version is pronounced.
In addition to the listed types of lambdacism, sonor [L] may be completely absent in speech. There is also a lower variant of pronunciation, in which the tip of the tongue does not rise upward. In the latter case, the sound is not distorted, so such a violation may not be corrected. Paralambdacisms include replacements of [L] with [Н], [У], [В], [J], [Р].
Treatment of lambdacism at the multidisciplinary center “Academy of the XXI Century. Speech.Intelligence”
When faced with such a problem as lambdacism, there is no need to be ashamed of it, much less let it take its course. Modern treatment methods, qualified specialists, an individual approach to each client and a comprehensive examination of the multidisciplinary center “Academy of the XXI Century. Speech.Intellect” will help to cope with this task. Our main specialist and project manager, Danilkina Margarita Yurievna, is a hereditary defectologist, a famous speech therapist, neuropsychologist, oligophrenopedagogue, specialist in the development of intelligence, rehabilitation, diagnosis and correction of developmental disorders in children and adults, the author of unique methods for the development of children in conditions of sensory-emotional play expansion and advanced development, professor, full member of the European Academy of Natural Sciences (Hannover).
There are no unsolvable problems, there are just lazy specialists. Professor Danilkina Margarita Yurievna has many scientific works on very complex diagnoses. Giving lectures at various universities around the world and conducting practical work. New techniques allow you to achieve amazing results.
Contact us at the center and you will see that together we can handle mountains.
Diagnostics
The task of determining the causes and type of lambdacism is implemented during speech therapy diagnostics. If it is necessary to clarify the medical aspects of the pathology, consultations with a pediatric dentist, maxillofacial surgeon, neurologist, or otolaryngologist are prescribed. To study speech status, the following is carried out:
- Examination of peripheral speech organs.
The speech therapist visually assesses the structure of the tongue, palate, lips, and pays attention to muscle tone. The child is asked to perform certain exercises that allow him to judge the mobility of the speech organs, the accuracy and switchability of movements. As part of such an examination, possible causes of lambdaism are established and a diagnostic hypothesis is put forward. - Analysis of phonemic hearing.
Necessary for the purpose of differentiating lambdacism and paralambdacism. To test speech hearing, speech therapy techniques of repetition, naming, and demonstration are used. Phoneme discrimination is tested in syllables and words. - Assessment of the phonetic side of speech.
At this stage, the pronunciation of all sounds is checked: the type of lambdaism is determined, and accompanying sound defects are identified. Based on the examination results, a plan and sequence of correction are outlined.
Articulation gymnastics
Automation of the sound "L"
To fix the sound after at least a month of work, you need to use the following methods:
- Pronounce soft syllables and words. For example: “Lyu: cradle, people, love.”
- Learn and speak simple phrases. “LE-LE-LE – leaves were lying on the ground” and others. You can compose them yourself.
- Come up with and repeat funny poems and tongue twisters starting with “L”.
- When a sound is produced in direct syllables, you need to fix it in reverse ones. OL, EUL, etc.
Be sure to control the position of your tongue in the mirror. And do not overload the texts with words with the letter “R”. The child must focus on one complex sound.
Automation of the hard “L” occurs by analogy. First, the child repeats after the adult, then does the exercises himself.
The exercises suggested above can be done independently at home. But if there is no improvement, you should definitely go to a speech therapist.
Correction
Health care
The participation of medical specialists may be required in case of lambdacism caused by dental problems, neurological pathologies (cerebral palsy), or hearing loss. Thus, with a shortened frenulum, in some cases, preliminary frenuloplasty is necessary, and with a cleft palate, uranoplasty is necessary. Hearing loss requires adequate selection of hearing aids. In case of a violation of muscle innervation, speech therapy work is preceded by a complex of medication, physiotherapeutic treatment, and massage.
Speech therapy assistance
Before starting to establish standard sound pronunciation, preparatory work is carried out to form the correct articulatory posture and develop phonemic hearing. At the first stage of correction of lambdacism, the following speech therapy techniques are used:
- Articulation gymnastics.
Includes exercises for developing the circular muscles of the lips (“Smile”, “Tube”), muscles of the tongue (“Needle”, “Watch”), stretching the hyoid ligament (“Horse”, “Mushroom”), developing the upper position of the tongue (“Painter” , “Swing”, “Turkey”), etc. It is also necessary to pay attention to the correct speech exhalation (exercise “Steamboat”). - Practicing basic sounds.
The supporting phonemes for [L] are [T] - gives the correct position of the tongue and [Y] - ensures the correct supply of the air stream. - Speech therapy massage.
Indicated for insufficient tongue mobility, weakness of the tip and lateral edges, spasticity of the back. Typically, such problems are observed with dysarthria. The most effective in this case is probe logomassage.
Sound production begins after completion of the preparatory stage. For various forms of lambdacism, differentiated methods and techniques are used: by imitation, based on basic sounds, using staged probes.
As soon as the sound [L] is received, they move on to consolidating it in syllables (direct, reverse, with a combination of consonants), words, phrases, stories. The differentiation stage is only necessary in cases of paralambdacity. The duration of correctional speech therapy sessions depends on the cause and mechanism of lambdaism, the presence of other phonetic defects that need correction.
Correction of lambdacism and rhotacism in primary schoolchildren with dyslalia
Primary school age is a period of development when correct speech is of particular importance for the formation of literacy. Among the most common manifestations of dyslalia in primary schoolchildren are lambdacism and rhotacism as violations of the pronunciation of sonorous sounds. Rotacism and lambdacism are violations of the pronunciation of the sounds r and l, respectively. Violations of sound pronunciation with normal hearing and intact innervation of the speech apparatus are called dyslalia. Dyslalia is one of the most common speech defects. According to A.G. Arushanova, sound pronunciation defects are observed in 15-25% of preschool children and 5-7% of primary schoolchildren [1].
The relevance of the issues of correction of labdacism and rhotacism is related to the fact that younger schoolchildren with dyslalia suffer from written speech, and as a result, poor academic performance is manifested. Younger schoolchildren mostly write as they speak. A close connection has been established between the clarity of the sound of children's speech and spelling literacy. Children with speech impediments may become withdrawn, shy, and may develop negativism. In classical speech therapy, when correcting sound pronunciation, the recommendations of M.E. are used. Khvattseva. During initial automation, the sound should be at the beginning of the word under stress in combination with a sound that is similar in articulation: [l] - in combination with [a] and [s]; [p] – after [t] and [d]; in such positions, sounds are more easily automated [7]. Then children learn to pronounce sounds in any combination.
M.F. Fomicheva clarifies that sounds in speech are not used in isolation. You should start automating sound with straight syllables, because the child has the opportunity to create the desired consonant articule and move to the vowel. First, a straight syllable with a vowel [a] is given, since when pronouncing it the lips are in a neutral position, the mouth is wide open, the tongue is in a lower position, which does not interfere with the articulation of the automated sound. Then they automate the sound with the vowel [s]. This is also a non-labialized sound and has less influence on the previous consonant. Next are syllables with [o] and [y]. Straight syllables in combination of a consonant with a vowel [e] are usually not used, because they are not typical for the Russian language and are found mainly in borrowed words (“mayor”, “sir”, etc.). The sound is then fixed in reverse syllables. Next, it is recommended to fix the sound in an intervocalic position (between two vowels) and, finally, in syllables with a cluster of consonants [6].
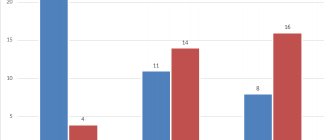
According to T.B. Filicheva, after automating the pronunciation of sounds in syllables, further work should be carried out in a strict sequence: automation of sounds in words (at the beginning of the word, middle, end); automation of sound in a sentence; automation of sound in pure sayings and poetry; automation of sounds in short, then long stories; automation of sounds in spoken speech [5]. We conducted a study of the manifestations of rhotacism and lambdacism in primary schoolchildren with dyslalia. According to a speech therapy examination, 55% of children with dyslalia had some kind of disturbance in sonorant sounds. Violation of hard [l] occurred in 20% of children, hard and soft [r] - in 40%. Note that one of the children has impaired pronunciation of both [p] and [l]. There were no single-stress pronunciations or pararotacisms. 2 children each display throaty, soft, lateral pronunciation; nasal pronunciation was found in only 1 of the children (12.5% of the group with rhoticism). The sound [r] is missing in one of the children (in addition to this type of rhotacism, he has impaired pronunciation of [l] and also has impaired pronunciation of whistling sounds). Among the lambdacisms in the group, the most common variants were found - replacements with in and short y. Impaired pronunciation of l in the form of lengthening of adjacent vowels occurred in a child with multiple sound pronunciation impairments.
Taking into account the importance of correct sound pronunciation for mastering literate speech and writing in primary schoolchildren, work was carried out to correct rhotacism and lambdacism, which included four main stages of correction of the disorders in question: preparatory, sound production, sound automation and, in cases of replacing one sound with another or mixing them, stage of differentiation.
When organizing and conducting correctional work, we used the recommendations of such researchers as M.I. Begun, L.N. Efimenkova, E.F. Sobotovich, T.B. Filicheva, M.F. Fomicheva, M.E. Khvattsev.
At the stage of preparatory exercises, the speech-auditory and speech-motor analyzers were prepared for the correct perception and reproduction of sound. The work was carried out in several directions: the formation of precise movements of the organs of the articulatory apparatus, a directed air stream, the development of fine motor skills of the hands, phonemic hearing, and the development of reference sounds
When correcting deficiencies in the sound pronunciation of the sound [p], exercises were used to develop the strength and tension of the air stream, an exercise for the lips. At the same time, they mainly offered active preparatory exercises. The goal of the sound production stage is to achieve the correct sound of an isolated sound.
Contents of the work: combining the movements and positions of the organs of the articulatory apparatus worked out at the preparatory stage and creating an articulatory base for a given sound, adding an air stream and voice (for sonorant and voiced ones), practicing the pronunciation of an isolated sound.
With rhotacism and lambacism, work, depending on the individual characteristics of the manifestation of the disorder, was carried out in the following ways: by imitation, from a reference sound, and also in a mixed way.
The next stage is to consolidate the given sounds and introduce them into speech (automation of the given sounds). The goal of this stage is to achieve the correct pronunciation of sounds in phrasal speech.
Children with dyslalia have incorrect stereotypes of pronunciation of sounds in various speech materials. Therefore, automation of sound requires the active use of the process of internal inhibition, the ability to differentiate correct and incorrect articulation patterns. It is carried out according to the principle “from simple to complex”. First of all, the inclusion of sound in syllables is carried out. A syllable is the simplest speech unit. Syllables do not matter, and therefore the child does not have stereotypes in the pronunciation of syllables, and this makes them easier to automate.
Certain requirements were imposed on the lexical material in relation to semantics. Speech material (words, phrases) was selected so that it was accessible to the child and, if possible, borrowed from everyday life, and then a vocabulary more complex in semantics was used.
First, sounds were introduced into two- and three-syllable words with straight syllables. Then they moved on to words with a reverse syllable. And only then did they move on to one- and two-syllable words with a combination of consonants at the beginning of the word. Gradually, words with fixed sounds are introduced into phrases in other contexts [2].
Experimental studies by E.F. Sobotovich showed that the process of forming and consolidating the correct pronunciation of sounds in words proceeds differently in children with the same types of sound pronunciation disorders. A correlation was discovered between the process of restructuring sound pronunciation reflexes, automation and their level of general speech development. In children with a high and normal level of speech formation, automation processes in any variant of the phonetic context proceed without difficulty. In children with a low level of speech formation, due to insufficiently formed phonemic hearing , automation is difficult. The author emphasizes that the process of perception and pronunciation of individual sounds and simple syllable combinations is largely more elementary compared to the process of forming and consolidating the correct pronunciation of words, and, consequently, the perception of various sounds included in a word, and correct placement them inside the word [4].
The goal of the sound differentiation stage is to teach children to distinguish between mixed sounds and to use them correctly in their own speech. Contents of the work: gradual, consistent differentiation of mixed sounds according to motor and acoustic characteristics, first isolated, then in syllables, words, sentences, phrases, poems, stories and in independent speech.
At the last stage of differentiation of the newly produced sound with the sound that is used as its substitute, differential inhibition was used. To fully use the skills of correct pronunciation of sounds, it is necessary to have phonemic hearing, i.e. the ability to distinguish speech sounds both in the pronunciation of another person and in one’s own speech.
Thus, the goal of speech therapy in correcting rhotacism and lambdacism is to correct the incorrect use of sounds in all types of speech activity: in oral, written, memorized and independent speech, in the process of play, study, social and industrial life. When correcting rhotacisms and lambdacisms at the preparatory stage, the child is offered a set of dynamic exercises. Sound production is carried out using the same technology for both rhotacisms and pararotacisms. When fixing a sound, it is important to follow a certain sequence. First, the sound is fixed in syllables, then in words and, finally, in phrases. To consolidate the sound in words, pictures are used in the names of which it is in different positions. First of all, the sound is practiced at the beginning of the word, then at the end and then in the middle. The task of fixing a sound also includes work to distinguish between a newly evoked sound and a sound that is similar in articulation or sound, in particular, [p] and [l].