Dyslalia and dysarthria are very similar speech development disorders. In both cases, there is a defect in sound pronunciation, often in the same phonemes
It is very rare that an ordinary person, simply by reading about these disorders on the Internet, will correctly distinguish one from the other. Meanwhile, it is important to know how dyslalia differs from dysarthria, since treatment and correction in both cases are individual.
What disorders occur only with dysarthria?
In differential diagnosis, dysarthria differs in leading features. So, this disease is characterized by the following symptoms, which do not appear with dyslalia:
● neurological pathogenesis, expressed in the form of asymmetry of the face, tongue, open mouth with lip paresis, smoothed nasolabial fold
● motor skills disorders - general, fine, speech
● voice defects - constriction, dull sound, slurredness (“mess in the mouth”)
● reduced speech activity
● deviations in diaphragmatic speech breathing, which causes prosody and automation of phonemes
● sleep disorders
● problems with memory capacity, instability of attention, intelligence, history of mental retardation, mental retardation.
● weak activity. People with dysarthria are usually slow and have difficulty switching from one activity to another.
● behavioral disorders - frequent mood swings, psychosis.
Differential diagnosis of dysarthria according to the degree of damage
In 96% of cases of dysarthria, the pseudopseudobulbar form of speech disorder occurs. Pseudobulbar dysarthria is differentiated by the degree of damage. The third, mild degree of dysarthria occurs with unilateral damage to the dominant hemisphere, most often the left, lower part of the anterior central gyrus. Patients experience the following changes in neurological status:
- Selective central cortical paresis of the muscles of the articulatory apparatus (usually the tongue). This leads to a limitation in the volume of the most subtle isolated movements. It is especially difficult to lift the tip of the tongue upward;
- Selective increase in muscle tone, which is most often concentrated in the muscles of the tip of the tongue;
- Violation of tempo and fluency of pronunciation.
Pronunciation becomes slow. Cakuminal consonants (Р, Ш, Ж,) are absent or replaced by dorsal ones (З, С, 3, СВ, ЗВ, Н, Т, Д). L and L often suffer.
Dysarthria of the second, moderate severity, occurs with unilateral damage to the cortex of the dominant hemisphere of the cortex in the lower postcentral parts of the cerebral cortex. Kinetic praxis deficiency develops (inability to produce a series of speech sounds). The patient is forced to look for the desired articulatory pattern, which slows down the pace and makes it difficult to speak fluently. He experiences difficulties in feeling and reproducing individual articulation patterns. Insufficiency of facial gnosis (the ability to recognize objects by sensory perceptions) develops, especially in the area of the articulatory apparatus. The child cannot accurately touch certain areas of the face.
The pace of speech is slowed down, and fluency suffers due to the search for articulation patterns. Speech becomes strained due to difficulty producing a series of sequential movements. Pronunciation is slow, but disturbances in the pronunciation of sounds are ambiguous and inconsistent. The pronunciation of hissing sounds (Shch, Sh, Zh) and affricates (C, Ch,) most often suffers. Sounds are difficult to automate. Speech remains blurred and unclear for a long time.
Severe dysarthria of the first degree is characteristic of damage to the lower parts of the premotor areas of the cerebral cortex. Patients have difficulty reproducing a series of sequential movements. There is a lack of kinetic dynamic praxis. In this regard, children experience great difficulty in automating given phonemes (speech sounds), especially words with a combination of consonants. Speech becomes strained due to difficulty producing a series of sequential movements. Affricates break up into parts: C into TS, Ch into TY and Sh. Frictional sounds are replaced by stop sounds S - G, 3 - D. When consonants coincide, the sounds are omitted. A person selectively deafens voiced consonants, mainly stops.
What is the difference between dysarthria and dyslalia?
According to its etiology, dysarthria is not an independent disorder. Its appearance is associated with congenital or acquired organic lesions of the central nervous system. It manifests itself in injuries, cerebral palsy, neuroinfections, problems with cerebral circulation, tumors, asphyxia, Rh conflict with the mother, and so on. Dyslalia is not associated with organic matter. It occurs:
• in somatically weakened children
• with pedagogical neglect
• with abnormal development of the articulatory apparatus.
In the case of dysarthria, the pronunciation and prosodic aspects of the sound flow suffer, omissions and phonemic substitutions are observed. With dyslalia, problems are expressed only in sound pronunciation.
Comparative analysis of dyslalia and erased dysarthria
Elena Uzlova
Comparative analysis of dyslalia and erased dysarthria
Dyslalia (from the Greek dis - a prefix meaning partial disorder, and lalio - I say) is a violation of sound pronunciation with normal hearing and intact innervation of the speech apparatus.
Among the violations of the pronunciation aspect of speech, the most common are selective violations in its sound (phonemic)
formalization during the normal functioning of all other operations of the statement.
These disorders manifest themselves in defects in the reproduction of speech sounds: distorted (abnormal)
their pronunciation, replacing some sounds with others, mixing sounds and, less often, omitting them.
The term " dyslalia "
One of the first in Europe to introduce it into scientific circulation was Vilnius University professor doctor I. Frank. In a monograph published in 1827, the study of this problem in domestic speech therapy is reflected in the works of: M. E. Khvattsev, A. M. Smirnova, O. V. Pravdina, S. S. Lyapidevsky, R. E. Levina and others no less famous scientists.
Dyslalia is one of the most common pronunciation defects. Statistical data from domestic and foreign researchers indicate that pronunciation deficiencies are present in 25-30% of preschool children (5-6 years old, 17-20% of school-age children (grades I-II)
. For older students, pronunciation deficiencies account for no more than 1%. This indicates that there are temporary disturbances that are overcome during the speech development of children and in the process of schooling.
The causes are biological and social: general physical weakness of the child due to somatic diseases, especially during the period of active speech formation; delayed mental development (minimal brain dysfunction, delayed speech development, selective impairment of phonemic perception; unfavorable social environment that impedes the development of child communication (limited social contacts, imitation of incorrect speech patterns, as well as educational deficiencies when parents cultivate imperfect child pronunciation, thereby delaying he is developing sound pronunciation).
There are two main forms of dyslalia , depending on the location of the disorder and the reasons causing the defect in sound pronunciation; functional and mechanical (organic)
.
In cases where there are no organic disorders (peripherally or centrally caused), we speak of functional dyslalia . In case of deviations in the structure of the peripheral speech apparatus (teeth, jaws, tongue, palate)
they talk about mechanical
(organic) dyslalia .
Functional dyslalia occurs in childhood during the process of mastering the pronunciation system, and mechanical dyslalia occurs at any age due to damage to the peripheral speech apparatus. With functional dyslalia , the reproduction of one or several sounds may be impaired; with mechanical dyslalia, a group of sounds usually suffers. In some cases, combined functional and mechanical defects occur.
Functional dyslalia . This includes defects in the reproduction of speech sounds (phonemes)
in the absence of organic disturbances in the structure of the articulatory apparatus.
With functional dyslalia, there are no organic disorders of the central nervous system that impede movement. The specific speech skills to voluntarily assume the positions of the articulatory organs necessary for pronouncing sounds are unformed. This may be due to the fact that the child has not developed acoustic or articulatory patterns of individual sounds. In these cases, it turns out that they have not learned one of the signs of a given sound. Phonemes do not differ in their sound, which leads to the replacement of sounds. The articulatory base turns out to be incomplete, since not all auditory motor formations (sounds)
formed. Depending on which of the signs of sounds - acoustic or articulatory - turned out to be unformed, sound replacements will be different.
In other cases, the child has formed all articulatory positions, but does not have the ability to distinguish between some positions, that is, to correctly select sounds. As a result, phonemes are mixed, the same word takes on a different sound form. This phenomenon is called mixing or interchange of sounds (phonemes)
.
Cases of abnormal sound reproduction due to incorrectly formed individual articulatory positions are often observed. The sound is pronounced as unusual in the phonetic system of the native language in its acoustic effect. This phenomenon is called sound distortion.
Mechanical dyslalia - impaired sound pronunciation caused by anatomical defects of the peripheral speech apparatus (organs of articulation)
. It is sometimes called organic. The most common pronunciation defects are caused by:
1) anomalies of the dentofacial system: diastema between the front teeth;
2) absence of incisors or their anomalies;
3) irreparable position of the upper or lower incisors or the relationship between the upper or lower jaw (bite defects)
.
These abnormalities may be due to developmental defects or acquired due to injury, dental disease or age-related changes. In some cases, they are caused by the abnormal structure of the hard palate (high vault)
.
Among pronunciation disorders in such cases, defects in whistling and hissing sounds are most often observed (they acquire excess noise, labiodental, anterior lingual, plosive, and less often - r and r.
Quite often, the pronunciation of vowel sounds is also disrupted, which become inaudible due to excessive noise in consonants and insufficient acoustic opposition of vowels.
However, dental anomalies do not always lead to pronunciation defects: with some deformation of the teeth, it may turn out to be normal.
The second most common group is made up of sound pronunciation disorders caused by pathological changes in the tongue: too large or small a tongue, shortened hyoid ligament.
With such anomalies, the pronunciation of sibilants and vibrants suffers, and lateral sigmatism is also observed. In some cases, the intelligibility of pronunciation as a whole suffers.
However, not all cases of language anomalies affect the pronunciation of sounds. This has been noted many times by linguists. (R. O. Yakobson, M. V. Panov)
and specialists in the field of speech pathology
(G. Gutzman, R. A. Yurova, etc.)
.
Facts of normal sound pronunciation with anomalies of the tongue and teeth indicate compensatory possibilities that make it possible to form a normal pronunciation even under impaired conditions for the realization of sounds; the same acoustic effect can be achieved in different ways.
Sound pronunciation disorders caused by labial anomalies are much less common, since congenital defects (various deformities)
overcome surgically at an early age.
Thus, the speech therapist encounters mainly the consequences of deformations of traumatic origin, in which the pronunciation of labial sounds is mainly impaired due to incomplete closure of the lips, as well as labiodental sounds. Sometimes there are defects in the pronunciation of labialized vowels (o, u)
.
Mechanical dyslalia can be combined with functional phonemic dyslalia.
In all cases of mechanical dyslalia, consultation is necessary (and in some cases treatment)
surgeon and orthodontist.
The term “
erased ” dysarthria was first proposed by O. A. Tokareva, who characterizes the manifestations of “
erased dysarthria ” as mild
(
erased ) manifestations of pseudobulbar
dysarthria , which are particularly difficult to overcome.
A different definition of such a speech disorder was proposed by A. N. Kornev. He defines this disorder as selective, mild, but rather persistent disturbances of sound pronunciation, which are accompanied by mild, peculiar disturbances of the innervation insufficiency of the articulatory organs.
Erased dysarthria (mild dysarthria , MDD - minimal dysarthric disorders ) in speech therapy practice is one of the most common and difficult to correct disorders of the sound-pronunciation side of speech.
A study of the neurological status of children with erased dysarthria reveals certain abnormalities in the nervous system, manifested in the form of a mildly expressed predominant unilateral syndrome. Paretic symptoms are observed in the articulatory and general muscles, which is associated with a violation of the innervation of the facial, glossopharyngeal or hypoglossal nerves (G. V. Gurovets, S. I. Mayevskaya)
.
Erased dysarthria occurs very often in speech therapy practice. The main complaints with erased dysarthria : slurred, inexpressive speech, poor diction, distortion and replacement of sounds in words with a complex syllable structure, etc.
Erased dysarthria is a speech pathology , manifested in disorders of the phonetic and prosodic components of the speech functional system and arising as a result of unexpressed microorganic damage to the brain (L. V. Lopatina)
.
Diagnosis of erased dysarthria and methods of correction work have not yet been sufficiently developed. The works of G. G. Gutsman, O. V. Pravdina, L. V. Melekhova, O. A. Tokareva, R. I. Martynova discuss the symptoms of dysarthric speech disorders , in which “washiness”
,
“
erased ” articulation.
The authors note that erased dysarthria is very similar in its manifestations to complex dyslalia . The works of L. V. Lopatina, N. V. Serebryakova, E. Ya. Sizova, E. K. Makarova and E. F. Sobotovich raise issues of diagnosis, differentiation of training and speech therapy work in groups of preschool children with erased dysarthria .
Among the causes of erased dysarthria , various authors have identified the following:
1. Violation of the innervation of the articulatory apparatus, in which there is a deficiency of individual muscle groups (lips, tongue, soft palate)
; inaccuracy of movements, their rapid exhaustion due to damage to certain parts of the nervous system.
2.Motor disorders: difficulty finding a certain position of the lips and tongue necessary to pronounce sounds.
3. Oral apraxia.
4. Minimal brain dysfunction.
The anamnesis of children with erased dysarthria , Mastyukova, Lopatina, Arkhipov, Karelin, etc., reveals the following factors: unfavorable course of pregnancy; asphyxia, low Apgar score at birth, the presence of a diagnosis of PEP - perinatal encephalopathy - in the vast majority of children in the first year of life.
How to correctly diagnose a speech disorder
The most important advice in a situation of problematic speech communication is not to listen to girlfriends, neighbors, acquaintances, that is, “it happened to me.” Perhaps it was, but in each case the violations occur in an individual form. Moreover, avoid visiting grandmothers who “pour out their voices.” Usually there is unsanitary conditions and a minimum of medical skills. If someone experienced improvements after such meetings, this is a coincidence. No slander, killed roosters, etc., are in any way connected with speech, much less, they do not recognize the differences between dyslalia and dysarthria.
To specify the diagnosis, you need to contact a qualified speech therapist. There are such specialists in every city. After a complete examination, he may also send you to a neurologist. A comprehensive examination is a necessity, not a waste of time. It is sometimes difficult to get a routine diagnosis without a referral, especially in small towns where there is only one doctor for the entire area. Therefore, take the opportunity to know exactly what your child is suffering from and how to treat it.
Causes of dyslalia:
- Features of the structure of the organs of the speech apparatus, the most common of which are malocclusion, short hyoid frenulum, high or low palate.
- Insufficient mobility of the organs of articulation, imprecision of movements or difficulties in switching from one position to another. In this case, the sounds are distorted. For example, instead of the correct sound “r”, the child pronounces “throat”, in the French manner, instead of the sound “l” - the sound “ue” .
- Lack of development of phonemic hearing and phonemic perception (the ability to recognize and distinguish speech sounds - phonemes). The child confuses similar sounds. At the same time, he experiences confusion or replacement of sounds. For example, “beetle” - “pike”, “fur coat” - “suba”, “shop” - “pakazin”, “paw” - “lyapa”.
- Imitation of incorrect speech of adults or children, excessive lisp, bilingualism.
Non-speech symptoms
1. Dyslalia Primary:- underdevelopment of the phonemic aspect of speech, underdevelopment of speech breathing (short exhalation, weak air stream).
Secondary:
- violations of written speech.
Not expressed Pronunciation of consonant sounds of late ontogenesis FN is impairedFFN
2. Rhinolalia Primary:- underdevelopment of the phonetic side of speech (omissions, distortion, replacement, confusion of sounds)
How to help a child?
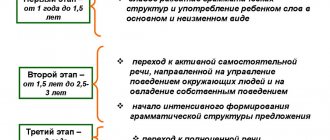
In the mechanical form, surgical correction of deficiencies of the speech organs is performed. The best time for this is under 7 years of age. After the tissue has healed, classes with a speech therapist begin. With a functional form, the neurologist prescribes a course of drug treatment, if necessary. Speech therapy assistance is carried out in several stages:
- development of auditory memory, formation of the ability to distinguish phonemes, for this purpose articulatory gymnastics, massage, speech motor skills are prescribed;
- production of sounds, memorization of them by the child. The exercises are based on the principle of imitation;
- development of communication skills.
With the age-related form, the child does not require special assistance, but parents need to closely monitor speech development. If after 6 years errors in the pronunciation of sounds have not disappeared, then this indicates a serious violation, you need to urgently visit a speech therapist.
FN
FFN
ONR
Comparative analysis of dyslalia, rhinolalia, dysarthria.
| p/p | Clinical and pedagogical classification definition | Etiology | Nature of damage to the vocal apparatus | Mechanisms | Forms. Subforms. | Degree of defect manifestation | ||
| Biological factors | Social and psychological factors | |||||||
| 1. | Dislalia | |||||||
Functional dyslalia
Causes:
- There may be an unfavorable speech environment.
- There may be incorrect speech education.
- There may be somatic weakness of health.
Neurological status of children:
- There are no neurological symptoms. Disorders from the autonomic nervous system may be observed, such disorders include: poor sleep, excessive sweating, pallor, bluishness of the skin or, conversely, their hyperemia.
Manifestation of neurological symptoms in fine motor skills:
- No.
Manifestation of neurological symptoms in facial muscles:
- No
In the organs of the articulatory apparatus:
- No
Mental status:
- Children with dyslalia do not have intellectual or emotional-volitional disorders.
State of household self-care skills:
- Neat and neat.
General somatic condition:
- Generally healthier.
Features of speech disorders:
- Sound disturbances occur primarily in the form of absence, replacement, i.e. phonological speech defects predominate.
- There are no prosody violations.
- Sound pronunciation does not deteriorate.
- The voluntary speech movements are preserved.
- According to the structure of the speech defect, the following can be observed: FNR (phonetic), FFNR, phonemic speech disorder.
- There are no violations of the lexico-grammatical aspect of speech.