Dysarthria is literally translated from Latin as “impairment of articulate speech.”
That is, there is incorrect pronunciation of words, which arises as a consequence of impaired innervation of the speech-motor apparatus. Erased dysarthria is a mild degree of the disorder. It manifests itself as mild speech defects, primarily in the phonetic and prosodic aspects of speech.
How it develops
Pathology occurs against the background of damage to the nerve fibers innervating the facial muscles. As a rule, in the erased form of the disease, the trigeminal, glossopharyngeal, hypoglossal and facial nerves are affected. This entails disruption of the components of the speech apparatus. The mobility of the lower jaw and lips is limited, the nasolabial fold is smoothed, and the activity of the soft palate, chewing and facial muscles is reduced. The amplitude of movement of the tongue, its retention of articulatory posture decreases, and its tremor develops.
In most cases, the disturbance of innervation is centralized. Based on this, several forms of erased dysarthria are diagnosed:
- cortical – formed when small pathological foci appear in the speech motor center. The phonetic, that is, pronunciation component of speech suffers;
- extrapyramidal - is formed when the subcortical nuclei and nerve ganglia are damaged and leads to a violation of speech prosody. That is, it loses its expressiveness;
- pseudobulbar - affects the pathways connecting the brain cortex with the nuclei of the cranial nerves. Causes a defect in both the phonetic and prosodic aspects of speech;
- mixed.
Erased dysarthria most often occurs in preschool children and is detected after 5 years. They cause a disorder in the pathology of perinatal, natal and postnatal development of the child. This includes pathological conditions during pregnancy: toxicosis and infectious diseases of the mother, intrauterine infections and fetal hypoxia.
Rapid or protracted labor, weak labor, cesarean section, Rh conflict, and birth trauma also influence the formation of pathology.
In the postnatal period, mainly in the 1st–2nd year of life, various diseases lead to the disorder: influenza, frequent acute respiratory viral infections, pneumonia, infectious processes and pathologies of the digestive tract, convulsive attacks against the background of hyperthermia, cerebral palsy, encephalopathy, hydrocephalic syndrome, perinatal damage to the central nervous system.
In adolescents, dysarthria in an erased form may be present starting from preschool age, or it may be acquired. Teenagers can acquire the disorder due to a brain injury or tumor, neuroinfections, or cerebrovascular accidents.
If dysarthria has developed in a child from an early age, then it is quite possible that he suffers from dysgraphia, that is, he is grammatically uneducated, and also has some problems with reading, perceiving and understanding speech. If the disease was acquired at an older age, then only a pronunciation defect is present. Written speech and understanding of what was said in relation to it is preserved.
Overcoming motor disorders in preschool children with dysarthria
“Scientific aspect No. 2-2019” – Humanities
UDC 376
Spiridonova Lyudmila Petrovna is a master’s student in the field of preparation “Special (defectological) education, profile “Speech therapy”” at the Faculty of Psychology and Pedagogy of Smolensk State University.
Scientific supervisor Elena Viktorovna Krylova – candidate of pedagogical sciences, associate professor of Smolensk State University.
Abstract: The article presents a theoretical analysis of the relationship between the development of motor skills and speech. The results of the ascertaining experiment are presented.
Key words: Speech development, dysarthria, motor disorders, articulatory motor skills.
Modernization of the preschool education system provides for a comprehensive comprehensive update of all links of the educational system in accordance with the requirements established by the Federal State Educational Standard for preschool education. One of the main objectives of the educational field “Speech Development”, highlighted in the Standard, is: mastery of speech by preschoolers as a means of communication and culture, development of coherent, grammatically correct dialogical and monologue speech, sound and intonation culture of speech. Currently, the number of children with one or another speech disorder is growing, which makes it difficult to implement the identified tasks.
One of the common speech disorders among preschool children is dysarthria, which is often combined with other speech disorders. This pathology manifests itself in disorders of the phonetic and prosodic components of the speech functional system, caused by insufficient innervation of the speech apparatus and resulting from organic damage to the central and peripheral nervous systems. [2, p. 62].
Available studies confirm the relationship between motor skills and speech (I.P. Pavlov, A.R. Luria, A.A. Leontyev, etc.). The formation of complex movements occurs with the participation of speech. And vice versa, precise, dynamic performance of exercises for the legs, torso, arms, and head prepares for the improvement of the movements of the articulatory organs - lips, tongue, lower jaw. Researchers note that children with dysarthria have a disorder not only of speech, but also of psychomotor development; they are characterized by some lag in the development of the motor sphere: poor coordination of movements, decreased speed and dexterity of their execution.
The theoretical analysis of materials on the research topic showed that the motor sphere is a set of motor capabilities (reactions, skills and abilities, complex motor acts) of a person, manifested in general motor skills, fine motor skills of the hands and fingers, articulatory motor skills, etc. . At different stages of a child’s development, his movements are not the same; they differ both in physiological parameters and in semantic characteristics. [3, p. 77].
The essence of motor development in normal ontogenesis lies in the simultaneous biologically determined maturation of the corresponding brain structures, and on this basis the child’s accumulation of individual motor experience, which he gains exclusively in the process of motor activity and verbal communication with other people. [4, p. 124].
Dysarthria is a speech disorder caused by organic damage to the central nervous system and is characterized by a combination of disturbances in the components of speech activity: articulation, diction, voice, breathing, facial expressions, melodic and intonation aspects of speech. Dysarthria is characterized by the presence of symptoms of organic damage to the central nervous system: insufficient innervation of the organs of articulation, disturbances in muscle tone in the articulatory and facial muscles (in the form of erased paresis). With dysarthria, various persistent violations of the phonetic aspect of speech are noted, which are leading in the structure of the speech defect, and deviations in the development of the lexico-grammatical structure of speech [1, p. 44].
The experimental study made it possible to identify the characteristics of the motor functions of preschool children with dysarthria. Analysis of medical documentation showed that all preschool children with dysarthria are exposed to pathological factors either during pregnancy and childbirth, or in the early stages of development.
A total of 20 children aged 5-6 years took part in the study.
The entire study sample was divided into experimental and control groups. The experimental group consisted of 10 preschool children with dysarthria. The control group consisted of 10 preschool children whose speech development corresponded to the age norm.
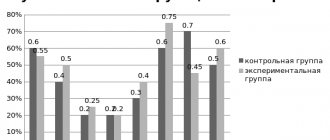
A study of the state of general motor skills showed:
| Indicators of development of general motor skills | Control group | Experimental group |
| Motor memory disorders | 20% | 70% |
| Switchability of movements and self-control | 20% | 50% |
| Lack of coordination in the movements of the arms and legs when marching | 10% | 50% |
| Delayed motor response | 20% | 60% |
| Impaired static coordination of movements (difficulty holding a pose, deviation of the body to the right and left, tremor of the eyelids and hands) | 10% | 80% |
| Impaired dynamic coordination of movements (inability to alternate steps and clap) | 10% | 40% |
| Impaired spatial coordination (uncertainty in completing tasks, lack of knowledge of the dominant hand) | 200% | 70% |
| Violations in the tempo of movements, slowing of movements, rhythmic sense (errors when reproducing a rhythmic pattern) | 10% | 50% |
In preschoolers with dysarthria, disorders of voluntary motor skills of the fingers (60%) were also revealed, which are manifested in poor quality of test performance, tension, stiffness of movements, the presence of synkinesis, hyperkinesis, as well as the inability to hold the thumb at a right angle to the palm, disturbances in the tempo of movement, exhaustion of movement. The completion of tasks by children in the control group, despite minor errors of 10%, turned out to be much higher.
An examination of the state of the motor skills of the articulatory apparatus of preschoolers with dysarthria showed that 30% of children have asymmetry in the innervation of the facial muscles, and symptoms of damage to the facial nerve are observed in the form of decreased sensitivity on the affected side and amicability. When studying the motor function of the lips, 70% of preschoolers noted the inability to raise the upper lip so that the upper teeth were visible, and lower the lower lip so that the lower teeth were visible.
When studying the motor function of the tongue, 80% of children were unable to place a wide tongue on the upper lip; the tongue was tense and moved back when opening the mouth, taking on a lumpy shape; In addition, tongue tremor was observed.
When studying the duration and force of exhalation, 70% of children had a shortened exhalation. A study of the dynamic organization of movements of the articulatory apparatus revealed the inability to differentiate movements, impaired smoothness of movements, tension of the tongue, hyperkinesis and synkinesis.
When studying the facial muscles and articulatory apparatus in preschool children with dysarthria, symptoms of rapid exhaustion and low quality of task performance were observed. In 60% of children, there was an inability to frown their eyebrows, raise them, feign surprise, wink, or puff out their cheeks alternately, while synkinesia and hyperkinesia were observed. Motor insufficiency manifested itself most clearly when performing complex motor acts.
It should be noted that preschoolers with normal speech development successfully coped with the tasks offered to them.
Thus, the modern educational system attaches great importance to the speech development of preschool children, but at the same time, the number of children suffering from speech disorders is increasing every year. One of the common speech disorders is dysarthria, characterized by the presence of symptoms of organic damage to the central nervous system: insufficient innervation of the articulatory organs, impaired muscle tone in the articulatory and facial muscles. Analysis of the results of the ascertaining experiment showed a violation of all indicators of the development of general, fine and articulatory motor skills in preschool children with dysarthria, which indicates the need for comprehensive speech therapy work to overcome the identified motor disorders.
Bibliography
- Arkhipova E.F. Erased dysarthria in children. – M.: Astrel, 2007. – 320 p.
- Belyakova L.I., Voloskova N.N. Dysarthria. – M.: Vlados, 2009. – 288 p.
- Bernstein HA On the construction of movements. – M.: Medicine, 2007. – 112 p.
- Bekhterev B.M. General basics of human reflexology. – St. Petersburg: Peter, 2009. – 228 p.
Interesting article? Share it with others:
Phonetic part of speech
With erased dysarthria, first of all, the pronunciation of sounds suffers, which is why the speech of such people is not entirely understandable for perception. However, there are forms of the disease in which speech defects are very modest and at first glance do not differ.
With this pathology, there is confusion, distortion, replacement or omission of individual sounds. First of all, those who require intervention from the tip of the tongue in their pronunciation suffer. The most significant sign, diagnosed in 80% of cases, is distortion of the pronunciation of the sound [r], in 65% of cases the sound [l] suffers. They are replaced by the child with sounds [th] or [g] that are easier to pronounce.
Interdental pronunciation of hissing and whistling sounds, for example, [zh], [sh], [z], [s], and deafening of voiced sounds are also common.
The interesting thing is that if these sounds are pronounced by a person in isolation, then no difficulties arise. But as soon as you include them in your speech, control is lost and their pronunciation is distorted. That is, it is difficult for such people to set them to automatic playback.
It has been established that most children with an erased form of dysarthria do not use many standard words in everyday life, confuse words that are similar in pronunciation, and when several consonants are combined in a word, they omit them.
The speech of dysarthric patients with a mild degree of disorder is blurred and not entirely intelligible.
Prosodic part of speech
In children and adolescents with mild dysarthric status, the prosodic side of speech also suffers. It characterizes melody, tempo and timbre, duration of pronunciation and determines the intelligibility and intelligibility of the speech pattern.
First of all, there is a lack of voice intonation. Children cannot read poetry expressively or change intonation aspects. They are unable to convey emotion intonationally, and their vocal range loses its breadth. Pauses between phrases are lost. There is a nasal tone to the voice. Narrative statements especially suffer. In general, speech becomes monotonous and inexpressive.
Due to the fact that with erased dysarthria, speech breathing slows down, exhalation is impaired, dysarthric people speak while inhaling. That's why they talk, as they say, excitedly.
The timbre of the voice directly depends on the emotional status. If the psychological status is dominated by inhibition processes
, then the voice becomes quiet, muffled, and acquires a hoarse or hoarse tone. Excitable dysarthrics have a ringing voice that turns into a scream.
The tempo of speech can also vary: for some it is accelerated, in which case the vowels fall out of the words, while for others it is slow, in which case the vowels, on the contrary, are overextended.
Speech also suffers rhythmically. It loses its emphasis, the emphasis in words is placed incorrectly. This affects the pronunciation, making it unusual and partially incomprehensible.
Other deviations
Disruption of the innervation of individual muscle groups not only upsets our usual speech patterns. The general appearance of the patient is also noteworthy. Noteworthy is the lack of facial expressions. The nasolabial fold and the corners of the mouth are asymmetrical. During speech activity, hypersalivation is a concern, since the ability to swallow saliva is impaired.
With paresis of the facial muscles, they lose tone. The lips and corners of the mouth are lowered, the tongue is inactive, and does not fully participate in word formation. Such features affect the intonation and expressiveness of the tale. Due to the weakness of the masticatory muscles, the lower jaw is not held in an elevated position, which is why the ability to keep the mouth closed is lost. Muscle weakness increases with articulatory load.
With a spasm of the facial muscles, there is no facial expression, the muscles are hard to the touch and tense. The lips seem to be constantly smiling due to a spasm of the upper lip. They practically do not participate in word formation. It is impossible to fold them into a tube or pull them forward.
Articulation suffers, the transition from one articulatory pose to another is disrupted. Autonomic disorders include sweating, cyanosis of the hands and feet.
Dysarthric people are able to perform almost all articulation tests: smile, puff out their cheeks, etc. However, their quality of execution noticeably suffers and is characterized by vagueness, blurriness, insufficient amplitude, and lethargy.
Such children are easily excitable, overly fussy, or, conversely, inhibited. Performance decreases, attention and memory suffer.
Difficulties arise in fine motor skills of the hands, as well as in general motor skills. During physical activity, children quickly get tired, it is difficult for them to maintain the rhythm and tempo of movements, or switch from one type to another.
Features of a child with erased dysarthria
Erased dysarthria occurs very often in speech therapy practice. The main complaints with erased dysarthria: slurred, inexpressive speech, poor diction, distortion and replacement of sounds in words with complex syllable structure, etc.
Erased dysarthria is a speech pathology that manifests itself in disorders of the phonetic and prosodic components of the speech functional system and arises as a result of unexpressed microorganic damage to the brain (L.V. Lopatina).
A survey of children in mass kindergartens showed that in senior and preparatory school groups from 40 to 60% of children have deviations in speech development. Among the most common disorders: dyslalia , rhinophonia, phonetic-phonemic underdevelopment, erased dysarthria .
In groups for children with general speech underdevelopment, up to 50% of children, and in groups with phonetic-phonemic underdevelopment, up to 35% of children have erased dysarthria. Children with severe dysarthria need long-term, systematic individual speech therapy assistance. Speech therapists of specialized groups plan speech therapy work as follows: in frontal, subgroup classes with all children they study program material aimed at eliminating general speech underdevelopment, and in individual classes they correct the pronunciation side of speech and prosody, i.e. elimination of symptoms of erased dysarthria.
The erased form of dysarthria is most often diagnosed after five years. All children whose symptoms correspond to erased dysarthria are sent for consultation to a neurologist to clarify or confirm the diagnosis and to prescribe adequate treatment, because in case of erased dysarthria, the method of correctional work should be comprehensive and include: - medical intervention; — psychological and pedagogical assistance; - speech therapy work.
For early detection of erased dysarthria and proper organization of complex effects, it is necessary to know the symptoms that characterize these disorders. The examination of the child begins with a conversation with the mother and study of the child’s outpatient development chart. Analysis of anamnestic information shows that there are: deviations in intrauterine development (toxicosis, hypertension, nephropathy, etc.); asphyxia of newborns; rapid or prolonged labor. According to the mother, “the child did not cry right away; the child was brought in to be fed later than everyone else.” In the first year of life, many were observed by a neurologist and prescribed medication and massage. The diagnosis for up to a year was “PEP” (perinatal encephalopathy). The development of a child after one year, as a rule, is successful for everyone, the neurologist no longer observes these children, and the child is considered healthy. When examined in a clinic by a speech therapist, children aged 5-6 years with erased dysarthria reveal the following symptoms:
GENERAL MOTOR SKILLS. Children with erased dysarthria are motorically awkward, the range of active movements is limited, and the muscles quickly tire during functional loads. They stand unsteadily on one leg, cannot jump on one leg, walk along a “bridge,” etc. They imitate movements poorly: how a soldier walks, how a bird flies, how bread is cut, etc. Motor incompetence is especially noticeable in physical education and music classes, where children lag behind in tempo, rhythm of movements, as well as in switching movements.
FINE MOTOR SKILLS OF HAND. Children with erased dysarthria late and have difficulty mastering self-care skills: they cannot button a button, untie a scarf, etc. During drawing classes, they don’t hold a pencil well and their hands are tense. Many people don't like to draw. Motor clumsiness of the hands is especially noticeable during applique classes and with plasticine. In works on appliqué, difficulties in the spatial arrangement of elements can also be traced. Violation of fine differentiated movements of the hands is manifested when performing sample tests of finger gymnastics. Children find it difficult or simply cannot perform an imitation movement without outside help, for example, “lock” - put their hands together, intertwining their fingers; “rings” - alternately connect the index, middle, ring and little fingers with the thumb, and other finger gymnastics exercises.
During origami classes they experience great difficulties and cannot perform the simplest movements, because... both spatial orientation and subtle differentiated hand movements are required. According to mothers, many children under 5-6 years old are not interested in playing with construction sets, do not know how to play with small toys, and do not assemble puzzles.
School-age children in the first grade experience difficulties in mastering graphic skills (some experience “mirror writing”; substitution of letters “d” - “b”, vowels, word endings; poor handwriting; slow pace of writing, etc.).
FEATURES OF THE ARTICULATING APPARATUS. In children with erased dysarthria, pathological features in the articulatory apparatus are revealed. Pareticity of the muscles of the organs of articulation is manifested in the following: the face is hypomimic, the facial muscles are flaccid upon palpation; Many children do not maintain the closed mouth pose, because the lower jaw is not fixed in an elevated state due to laxity of the masticatory muscles; lips are flaccid, their corners are drooping; During speech, the lips remain flaccid and the necessary labialization of sounds is not produced, which worsens the prosodic aspect of speech. The tongue with paretic symptoms is thin, located at the bottom of the mouth, flaccid, the tip of the tongue is inactive. With functional loads (articulation exercises), muscle weakness increases. Spasticity of the muscles of the organs of articulation is manifested in the following: the face is amicable, the facial muscles are hard and tense on palpation. The lips of such a child are constantly in a half-smile: the upper lip is pressed against the gums. During speech, the lips do not take part in the articulation of sounds. Many children who have similar symptoms do not know how to perform the “tube” articulation exercise, i.e. pull the lips forward, etc. With a spastic symptom, the tongue is often changed in shape: thick, without a pronounced tip, inactive.
Hyperkinesis with erased dysarthria manifests itself in the form of trembling, tremor of the tongue and vocal cords. Tremor of the tongue appears during functional tests and loads. For example, when asked to support a wide tongue on the lower lip with a count of 5-10, the tongue cannot maintain a state of rest, trembling and slight cyanosis appear (i.e., blue tip of the tongue), and in some cases the tongue is extremely restless (waves roll through the tongue in longitudinal or transverse direction). In this case, the child cannot keep his tongue out of the mouth. Hyperkinesis of the tongue is often combined with increased muscle tone of the articulatory apparatus.
Apraxia with erased dysarthria is simultaneously detected in the inability to perform any voluntary movements with the hands and organs of articulation. In the articulatory apparatus, apraxia manifests itself in the inability to perform certain movements or when switching from one movement to another. Kinetic apraxia can be observed when the child cannot smoothly transition from one movement to another. Other children experience kinesthetic apraxia, when the child makes chaotic movements, “groping” for the desired articulatory position. Deviation, i.e. deviation of the tongue from the midline, also manifests itself during articulation tests and during functional loads. Deviation of the tongue is combined with asymmetry of the lips when smiling with a smoothness of the nasolabial fold.
Hypersalivation (increased salivation) is detected only during speech. Children cannot cope with salivation, do not swallow saliva, and the pronunciation side of speech and prosody suffer.
When examining the motor function of the articulatory apparatus in children with erased dysarthria, the ability to perform all articulation tests is noted, i.e. Children, according to instructions, perform all articulatory movements - for example, puff out their cheeks, click their tongue, smile, stretch out their lips, etc. When analyzing the quality of performing these movements, one can note: blurriness, unclear articulation, weakness of muscle tension, arrhythmia, decreased range of movements, short duration of holding a certain pose, decreased range of movements, rapid muscle fatigue, etc. Thus, under functional loads, the quality of articulatory movements sharply falls. During speech, this leads to distortion of sounds, their mixing and deterioration in the overall prosodic aspect of speech.
SOUND PRONUNCIATION. When first meeting a child, his sound pronunciation is assessed as complex dyslalia or simple dyslalia. When examining sound pronunciation, the following are revealed: confusion, distortion of sounds, replacement and absence of sounds, i.e. the same options as for dyslalia. But, unlike dyslalia, speech with erased dysarthria also has disturbances on the prosodic side. Impaired pronunciation and prosody affect speech intelligibility, intelligibility, and expressiveness. Some children go to the clinic after classes with a speech therapist. Parents ask why the sounds that the speech therapist provided are not used in the child’s speech. The examination reveals that many children who distort, omit, mix or replace sounds can pronounce these same sounds correctly in isolation. Thus, sounds in erased dysarthria are produced in the same ways as in dyslalia, but for a long time they are not automated and are not introduced into speech. The most common violation is a defect in the pronunciation of whistling and hissing sounds. Children with erased dysarthria distort and mix not only articulatory complex sounds that are close in place and method of formation, but also acoustically opposed ones. Quite often, interdental pronunciation and lateral overtones are noted. Children have difficulty pronouncing words with a complex syllabic structure; they simplify the sound content by omitting some sounds when consonants are combined.
PROSODICA. The intonation-expressive coloring of the speech of children with erased dysarthria is sharply reduced. The voice, vocal modulations in pitch and strength suffer, speech exhalation is weakened. The timbre of speech is disrupted and sometimes a nasal tone appears. The pace of speech is often accelerated. When reciting a poem, the child’s speech is monotonous, gradually becomes less intelligible, and the voice fades away. The children's voice during speech is quiet, modulation in pitch and voice strength is not possible (the child cannot change the pitch of the voice by imitation, imitating the voices of animals: cows, dogs, etc.). In some children, speech exhalation is shortened, and they speak while inhaling. In this case, speech becomes choked. Quite often, children are identified (with good self-control) in whom, during a speech examination, deviations in sound pronunciation do not appear, because They pronounce the words in a chant, i.e. by syllables, and only violation of prosody comes first.
GENERAL SPEECH DEVELOPMENT. Children with erased dysarthria can be divided into three groups. First group. Children who have impaired sound pronunciation and prosody. This group is very similar to children with dyslalia. Often, speech therapists treat them as dyslastic, and only in the process of speech therapy work, when there is no positive dynamics in the automation of sounds, does a suspicion arise that this is erased dysarthria. Most often, this is confirmed during an in-depth examination and after consultation with a neurologist. These children have a good level of speech development, but many of them have difficulty learning, distinguishing and reproducing prepositions. Children confuse complex prepositions and have problems distinguishing and using prefixed verbs. At the same time, they speak coherent speech and have a rich vocabulary, but may have difficulty pronouncing words with a complex syllabic structure (for example, frying pan, tablecloth, button, snowman, etc.). In addition, many children experience difficulties with spatial orientation (body diagram, concepts of “below-above,” etc.).
Second group. These are children in whom a violation of sound pronunciation and the prosodic side of speech is combined with the incomplete process of forming phonemic hearing. In this case, children encounter isolated lexical and grammatical errors in their speech. Children make mistakes in special tasks when listening and repeating syllables and words with oppositional sounds - for example, when asked to show the desired picture (mouse-bear, fishing rod-duck, scythe-goat, etc.).
Thus, in children, the auditory and pronunciation differentiation of sounds is unformed. Children's vocabulary lags behind the age norm. Many people experience difficulties in word formation, make mistakes in agreeing a noun with a numeral, etc. Sound pronunciation defects are persistent and are regarded as complex, polymorphic disorders. This group of children with phonetic-phonemic underdevelopment (FFN) and erased dysarthria should be referred by the speech therapist of the clinic to the MPC (medical-pedagogical commission), to a specialized kindergarten (to the FFN group).
Third group. These are children who have a persistent polymorphic disorder of sound pronunciation and a lack of prosodic aspect of speech combined with underdevelopment of phonemic hearing. As a result, the examination reveals a poor vocabulary, pronounced errors in grammatical structure, the impossibility of a coherent statement, and significant difficulties in mastering words of different syllabic structures.
All children in this group demonstrate undeveloped auditory and pronunciation differentiation. Ignoring prepositions in speech is indicative. These children with erased dysarthria and general speech underdevelopment (GSD) should be sent to MPC (in specialized kindergarten groups) to GSD groups. Thus, children with erased dysarthria are a heterogeneous group. Depending on the level of development of linguistic means, children are sent to specialized groups: - with phonetic disorders; - with phonetic-phonemic underdevelopment; - with general speech underdevelopment .
(according to E. F. Arkhipova)
Do you need a speech therapist in Sviblovo? Sign up for a consultation by phone or through the feedback form in the “Contacts” section.