Parents who have learned from specialists that their child has problems with speech development often wonder what causes them. This question becomes especially important for them if none of the immediate family had speech disorders. Speech disorders can arise under the influence of unfavorable circumstances, or, as experts say, harmful factors acting from within or without and often combined with each other.
Special and reference literature describes the causes predisposing to the occurrence of speech disorders. They are usually divided into two groups - organic (leading to disruption of mechanisms in the central or peripheral speech apparatus) and functional (disrupting the normal functioning of the speech apparatus).
It is worth practicing with children for any speech problems!
Speech disorders are said to occur if a child's speech skills do not correspond to his age. Many disadvantages are difficult to overcome on your own. Pedagogical science - speech therapy - helps to cope with them.
It’s worth remembering: no matter what childhood speech disorders are, they definitely need to be dealt with and not left to chance. Mild speech problems may disappear completely. With reasonable effort and practice, this will happen faster. Moderate and severe violations are subject to partial correction.
Hopeless cases occur only with complex defects of the articulatory apparatus, psyche or brain structures, but there are options here too.
The child will have to adapt to life in society, and our task is to help him do this as painlessly as possible. Intelligible, clear speech and the ability to formulate thoughts influence socialization. Although we try to fight it, children with speech disorders are often teased, we must try to avoid this. It is important that the child is understood by his peers and others, this affects his self-esteem and desire to adapt to society.
Types of speech errors
First, let's figure out what speech errors are. Speech errors are any cases of deviation from current language norms. Without their knowledge, a person can live, work and communicate normally with others. But the effectiveness of the actions taken in certain cases may suffer. In this regard, there is a risk of being misunderstood or misunderstood. And in situations where our personal success depends on it, this is unacceptable.
The author of the classification of speech errors given below is Doctor of Philology Yu. V. Fomenko. Its division, in our opinion, is the simplest, devoid of academic pretentiousness and, as a result, understandable even to those who do not have a special education.
Types of speech errors:
Where do speech disorders come from?
Speech disorders are problems with verbal communication, speech motor skills, and related areas. They are very diverse: some are associated with the inability to speak, others with speech incontinence. They arise due to physiological, neurological or mental problems, due to pedagogical neglect. Any speech disorder is not a reason to stigmatize a child, much less shame him.
Difficulties with speech can be organic, that is, caused by damage to the speech organs. They are like this:
- Hereditary, when the problem was passed on from parents. It happens that one of the parents at one time began to speak later, has peculiarities in the bite or setting of the teeth, and this is passed on to the children.
- Congenital (intrauterine) pathologies. Caused by the difficult course of pregnancy or taking medications, hypoxia, infectious disease of the pregnant woman, blood incompatibility, prematurity or postmaturity, maternal stress or intoxication.
- Perinatal (caused by complications during childbirth). Priority attention should be given to children who suffered asphyxia or head trauma due to a narrow birth canal, were born weighing less than 1.5 kg and were resuscitated.
- Postnatal (caused by diseases in the first months or years of life). Speech disturbances can cause infections (meningitis, otitis media), head injuries and palatal injuries.
- Social and everyday, when the child lacks emotional and verbal communication with loved ones. These are not necessarily families with drinking parents - it happens that quite successful mothers and fathers simply do not have enough time for their children.
Also, speech disorders can be of an endocrine nature (due to the characteristics of the child’s psychomotor development), functional (defects or characteristics of the speech organs), psychosomatic or caused by the environment.
Factors that can affect speech function
In the case of children, the formation of speech can be influenced by both factors that acted before birth, as well as intranatal and postnatal ones.
The following can lead to different severity of disorders:
- Fetal hypoxia in the intrauterine stage of development.
- Infectious diseases suffered by the mother during pregnancy or intoxication with various chemicals.
- The use of a number of medications during pregnancy can also lead to speech disorders.
- Birth trauma can also cause speech disorders.
- Asphyxia, low birth weight, and low Apgar score.
- Injuries, bruises and concussions can also cause such disorders.
- Speech disorders can also arise against the background of unfavorable social and living conditions in which the child finds himself.
- Imitating the incorrect speech of others.
What should parents be wary of in their child’s speech?
Symptoms of speech disorders can be different: a poor vocabulary (the baby does not remember words well, confuses endings, speaks little, uses generalizations), poor understanding of words or phrases, and inability to reproduce certain sounds. The most famous defect is stuttering, which disrupts the rhythm and fluency of speech.
According to experts, the problem can be identified very early. You need to communicate with your baby from the first moments of his life, even when he is not able to consciously react. If a child does not show similar communicative activity as other children of his age, you should pay attention. But this in itself is not a diagnosis; you don’t need to beat yourself up right away.
The features listed in the table may indicate problems with speech in children.
| Month of life (by the end of the month) | What the baby can't do |
| 1 | Doesn't cry when hungry or uncomfortable |
| 4 | Doesn't smile back when people talk to him |
| 5 | Does not produce sounds or sound combinations. Does not look for things that an adult is pointing at |
| 7 | Does not know how to attract the attention of adults using sounds |
| 9 | There are still no words consisting of two repeated syllables (ma-ma, ba-ba, na-na) |
| 10 | The child does not speak 8 syllables. Doesn’t shake his head in denial, doesn’t make a “bye-bye” gesture with his pen |
| 12 | Doesn’t say a word, doesn’t react to simple requests (“give me the ball”) |
| 15 | Can't even say "mom" or "dad" |
| 19 | Doesn't speak meaningful words. Doesn't point at body parts the parent is talking about |
| 29 | Doesn’t understand the difference between “big” and “small” |
The last indicator - the end of the 29th month - is close to the time when it is time for the child to go to kindergarten. Violations, if any, are already noticeable by this point. If these problems occur, you should visit a consultation:
- otolaryngologist (perhaps the baby speaks poorly because he cannot hear);
- neurologist (check for organic damage to the central nervous system, speech centers of the cerebral cortex);
- child psychologist, psychiatrist, defectologist (find out the state of the child’s non-verbal intelligence);
- speech therapist (will conduct a final diagnosis).
Reviews and comments
Now you can practice and find speech errors in this article or share other examples you know. Also, take a look at our literacy course.
We also recommend reading:
- Storytelling
- How to learn to speak beautifully
- Orthoepy - why it is important to speak correctly and how these rules arise
- Our. Native. Russian.
- How to independently learn to write correctly in Russian
- Learning a foreign language: old rules about the main thing
- Development of speech culture
- Recommendations for learning Russian
- Lukomorye, cat and literacy
- How to write correctly: 8 ways to improve literacy
- Learning your native language: a selection of useful materials
Keywords:_D1048, _D1049, 1Russian, 1Storytelling
Types of speech disorders (classification from a medical point of view)
Speech problems in preschool children can be classified according to clinical-pedagogical and psychological-pedagogical indicators. The two classifications should be considered together: together they help to understand the cause of the violation and determine ways to eliminate it.
The clinical and pedagogical classification is closer to the medical one, and we’ll talk about it now. She divides speech deviations into oral and written. The first can be phonational or systemic.
With phonation, the source of the problem can be improper voice formation, sound pronunciation, tempo, and intonation. That is, the child understands speech directed to him 100%, but cannot reproduce it. The following phonation disorders are classified (in alphabetical order):
- Bradylalia is a slow rate of speech.
- Dysarthria is a disorder due to insufficient innervation of the articulatory apparatus.
- Dysglosia - difficulties with pronunciation due to palatal, jaw, and other clefts.
- Dyslalia is a deviation with full hearing and intact speech apparatus.
- Dysphonia is a complete or fragmented disorder of phonation due to an abnormality of the vocal apparatus.
- Stuttering is a disruption in tempo due to spasms of the jaw muscles.
- Rhinolalia is a specificity of voice timbre and sound pronunciation due to articulatory features.
- Tahilalia - the child is frequent with words.
Systemic deviations are more severe. They are formed due to lesions in the cerebral cortex. The child partially loses the ability to correctly repeat words and phrases and understand their meaning. There are two types of violations:
- Alalia is the inability to speak or underdevelopment due to damage to the speech areas of the cerebral cortex formed during fetal development or after birth.
- Aphasia is a complete or partial loss of speech due to brain damage (stroke, etc.). More often, the diagnosis is made explicitly after the 3rd birthday.
Among the above, severe speech disorders can be identified - persistent deviations of the speech system with preserved hearing and intelligence. These include sensory and motor alalia, severe variants of dysarthria, rhinolalia, stuttering, aphasia and other deviations. Such problems can influence the formation of the psyche.
Impairments in written speech can be noticed in older kindergarten or in the first grades of school. This is dyslexia (the child incorrectly identifies letters and forms words from them, difficulties arise with reading), dysgraphia (when writing, letter signs are mixed, rearranged or omitted).
Article:
The term “etiology” is Greek and means the study of causes (etio - cause, logos - science, doctrine).
The problem of causality has long attracted the attention of mankind. The development of etiology as a doctrine of causes is closely related to the general scientific progress of a number of medical and natural disciplines. The concept of “etiology” is a philosophical category, so its connection with the development of philosophy is obvious. A great contribution to the solution of this problem was made by the research of the largest Russian pathophysiologist I.V. Davydovsky, who wrote: “Every true meaning goes back to reasons, that is, to the concepts of causality and determinism. These are two related but different concepts that treat, on the one hand, about causality, i.e., about cause-and-effect relationships (this should be the meaning of the concept “etiology”), on the other hand, about the knowledge of the essence, phenomenon, i.e. . laws that underlie it (determinism in the proper sense of the word).”
The problem of the etiology of speech disorders has followed the same path of historical development as the general doctrine of the causes of painful conditions.
Even in ancient times, the Greek philosopher and physician Hippocrates (460-377 BC) saw the cause of a number of speech disorders, in particular stuttering, in brain damage.
Another Greek philosopher Aristotle (384-322 BC), linking the processes of speech formation with the anatomical structure of the peripheral speech apparatus, saw the causes of speech disorders in disorders of the latter.
Thus, already in the research of ancient scientists, two directions emerged in understanding the causes of speech disorders. The first of them, coming from Hippocrates, gave the leading role in the occurrence of speech disorders to brain lesions; the second, originating from Aristotle, is disorders of the peripheral speech apparatus. At subsequent stages of studying the causes of speech disorders, these two points of view were preserved.
Ideas about the etiology of speech disorders at all stages and the study of this problem reflect an understanding of their essence, as well as the general methodological directions of a certain era and authors. Despite the fact that the assumption about the role of brain damage in the etiology of speech disorders was made four centuries BC. e. Hippocrates, truly scientific confirmation was given only in 1861, when the French physician Paul Broca showed the presence in the brain of a field specifically related to speech, and associated the loss of speech with its damage. In 1874, a similar discovery was made by Wernicke: a connection was established between understanding and the preservation of a certain area of the cerebral cortex. Since that time, the connection between speech disorders and morphological changes in certain parts of the cerebral cortex has become proven.
The issues of the etiology of speech disorders began to be developed most intensively in the 20s of this century. During these years, domestic researchers made the first attempts to classify speech disorders depending on the causes of their occurrence. Thus, S. M. Dobrogaev (1922) among the causes of speech disorders identified “diseases of higher nervous activity,” pathological changes in the anatomical speech apparatus, insufficient education in childhood, as well as “general neuropathic conditions of the body.”
M.E. Khvattsev was the first to divide all the causes of speech disorders into external and internal, especially emphasizing their close interaction. He also identified organic (anatomical-physiological, morphological), functional (psychogenic), socio-psychological and neuropsychiatric causes.
Organic causes included underdevelopment and damage to the brain in the prenatal period, at the time of childbirth or after birth, as well as various organic disorders of the peripheral speech organs. They identified organic central (brain lesions) and organic peripheral causes (damages to the organ of hearing, cleft palate and other morphological changes in the articulatory apparatus). M. E. Khvattsev explained the functional reasons He emphasized the interaction of organic and functional, central and peripheral causes. He included mental retardation, memory impairment, attention disorders and other disorders of mental functions as psychoneurological causes
M.E. Khvattsev also assigned an important role to socio-psychological reasons, understanding by them various unfavorable environmental influences. Thus, he was the first to substantiate the understanding of the etiology of speech disorders on the basis of a dialectical approach to assessing cause-and-effect relationships in speech pathology.
Great achievements in the field of biology, embryology, theoretical medicine over the past decades, advances in medical genetics, immunology and other disciplines have made it possible to deepen the understanding of the etiology of speech disorders and show the importance of exogenous (external) and endogenous (internal) harm in their occurrence. It is important not only to identify organic (central and peripheral) as well as functional causes of speech disorders, but also to imagine the mechanism of speech disorders under the influence of certain adverse effects on the child’s body. This is necessary both for the development of adequate ways and methods for correcting speech disorders, as well as for their prognosis and prevention.
The cause of speech disorders is understood as the impact on the body of an external or internal harmful factor or their interaction, which determine the specifics of a speech disorder and without which the latter cannot occur.
The question of the role of external and internal factors in the etiology of speech disorders is one of the sections of the general problem of causation. A close relationship has been established between these factors in the occurrence of speech pathology and in the formation of its clinical picture.
Social conditions and factors that promote or hinder the occurrence of speech disorders play an important role in the occurrence of speech disorders. For example, when a child stutters, mental trauma is considered as an external cause. Favorable conditions for the occurrence of stuttering may be the somatic weakness of the child, his neuropathic constitution (increased neuropsychic excitability), residual effects of early organic damage to the central nervous system, age, etc. In different cases, the same factor can play a role, either the conditions or the causes. Thus, in the above example, the age of the child, as favorable for the onset of stuttering (the stage of the most intensive development of speech), in combination with constitutional increased neuropsychic excitability, can become the cause of stuttering.
The basis for studying the etiology of speech disorders is the evolutionary-dynamic approach and the principle of dialectical unity of the biological and social in the process of formation of the psyche. In this aspect, the development of a child’s speech activity is determined by the degree of maturity of his central nervous system and largely depends on the characteristics of the child’s interaction with the outside world.
The concept of mental development, developed by L. S. Vygotsky, constitutes the methodological basis for studying the causes of speech development disorders in childhood. Emphasizing the connection between mental development and environmental influences, he introduced the concept of the social situation of development. It is a combination of internal development processes and external conditions that are specific to each age stage.
The maturation of the speech functional system is based on afferentation, i.e., the arrival from the outside world through various analyzers, primarily the auditory analyzer, of various signals and, above all, speech. The source of auditory afferentation is the adult who communicates with the child. In this regard, the role of the speech environment and speech communication is very large, and their insufficiency can be one of the main reasons that disrupts speech formation.
Young children raised in an environment with a limited or defective speech environment (deaf-mute parents or parents with speech defects, long-term hospitalization, limited social contacts due to various serious illnesses, for example, children with cerebral palsy) are lagging behind in speech development.
For normal speech development of a child, communication must be meaningful, take place against an emotionally positive background and encourage him to respond. It is not enough for him to simply hear sounds (radio, tape recorder, TV); first of all, he needs direct communication with adults based on the leading form of activity characteristic of this age stage. An important stimulus for speech development is a change in the forms of communication between a child and an adult. Thus, the replacement of emotional communication, characteristic of the first year of life, with objective-active communication at the age of 2-3 years is a powerful stimulus for the development of his speech. If this change in the nature of communication between an adult and a child does not occur, then a lag in speech development may occur.
A prerequisite for the development of speech is the child’s accumulation of impressions in the process of his object-based play activities, which create the basis for assimilating the meanings of words and forming their connection with images of objects in the surrounding reality.
The development of a child’s speech is delayed under unfavorable external conditions: lack of an emotionally positive environment, extremely noisy surroundings.
Speech develops by imitation, so some speech disorders (unclear pronunciation, stuttering, impaired speech tempo, etc.) may be based on imitation.
Speech disorders often occur due to various mental traumas (fear, feelings of separation from loved ones, long-term traumatic situation in the family, etc.). This delays the development of speech, and in some cases, especially with acute mental trauma, causes psychogenic speech disorders in the child: mutism, neurotic stuttering. These speech disorders, according to the classification of M. E. Khvattsev, can conditionally be classified as functional.
Functional speech disorders also include disorders associated with adverse effects on the child’s body: general physical weakness, immaturity due to prematurity or intrauterine pathology, diseases of internal organs, rickets, metabolic disorders.
Thus, any general or neuropsychic disease of a child in the first years of life is usually accompanied by a violation of speech development.
Hence, it is legitimate to distinguish between defects of formation and defects of formed speech, considering the age of three as their conditional division.
When assessing speech disorders in children, it is important to take into account the so-called critical periods, when the most intensive development of certain parts of the speech system occurs, and therefore there is an increased vulnerability of the nervous mechanisms of speech activity and the risk of disturbances in its function even when exposed to minor exogenous hazards. In these cases, a critical period in speech development is a predisposing condition for the occurrence of speech disorders.
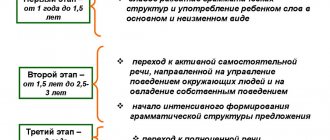
There are three critical periods in the development of speech function. The first (1-2 years of life), when the prerequisites for speech are formed and speech development begins, the foundations of communicative behavior are formed and the need for communication becomes its driving force. At this age, the most intensive development of cortical speech zones occurs, in particular Broca's area, the critical period of which is considered to be the child's age of 14-18 months. Any, even seemingly insignificant, unfavorable factors operating during this period can affect the development of the child’s speech.
The second critical period (3 years), when coherent speech intensively develops, a transition occurs from situational speech to contextual speech, which requires great consistency in the work of the central nervous system (speech motor mechanism, attention, memory, volition, etc.). A certain discrepancy that arises in the work of the central nervous system, in neuroendocrine and vascular regulation leads to a change in behavior, obstinacy, negativism, etc. are observed. All this determines the greater vulnerability of the speech system. Stuttering, mutism, and delayed speech development may occur. The child refuses verbal communication, and a reaction of protest appears to the excessive demands of adults on him.
Stuttering that occurs at this stage may be due to age-related unevenness in the maturation of individual parts of the speech functional system and various mental functions. In the literature, they are sometimes referred to as evolutionary, i.e., associated with the age phase of development: for example, “evolutionary stuttering.”
The third critical period (6 - 7 years) is the beginning of the development of written speech. The load on the child’s central nervous system increases. When increased demands are made, “disruptions” in nervous activity may occur with the appearance of stuttering.
Any disturbances in the child’s speech function manifest themselves most strongly during these critical periods; in addition, new speech disorders may arise. The speech therapist must be well aware of the critical periods in the development of a child’s speech and take them into account in his work.
Critical periods of speech development play the role of predisposing conditions; they can have either independent significance or be combined with other unfavorable factors - genetic, general weakness of the child, dysfunction of the nervous system, etc.
The dynamics of age-related speech development in the first years of life vary significantly depending on the genotype of the organism and the influence of the environment on it. For the development of the speech functional system, normal maturation and functioning of the central nervous system is necessary.
play a large role in the occurrence of speech disorders . This group of causes, according to the classification of M. E. Khvattsev, can be classified as organic central, in case of brain damage, and organic peripheral, if under the influence of various unfavorable intrauterine factors the morphological development of the peripheral speech apparatus is disrupted.
Exogenous -organic factors mean various adverse effects (infections, injuries, intoxications, etc.) on the child’s central nervous system and on his body as a whole. Depending on the time of exposure to these factors, intrauterine pathology is distinguished, or prenatal (exposure during intrauterine development); damage during childbirth (catal pathology) and exposure to various harmful factors after birth (postnatal pathology). Intrauterine pathology is often combined with damage to the child’s nervous system during childbirth. This combination in modern medical literature is referred to as “perinatal pathology”. Such lesions of the nervous system combine various pathological conditions caused by exposure of the fetus to harmful factors in the prenatal period, during childbirth and in the first days after birth. Perinatal pathology can be caused by diseases of the mother during pregnancy, infections, intoxications, toxicosis of pregnancy, as well as a variety of obstetric pathologies (narrow pelvis, prolonged or rapid labor, premature rupture of water, entanglement of the umbilical cord, malpresentation of the fetus, etc.). Obstetric manipulations are also important, which can damage the fetal nervous system.
occupy a leading place in the perinatal pathology of the nervous system .
The occurrence of intracranial birth trauma and asphyxia (oxygen starvation of the fetus at the time of birth) is facilitated by disruption of intrauterine development of the fetus. Birth trauma and asphyxia aggravate developmental disorders of the fetal brain that occur in utero. Birth trauma leads to intracranial hemorrhage and death of nerve cells. Intracranial hemorrhages can also involve the speech zones of the cerebral cortex, which entails various speech disorders of cortical origin (alalia). In premature babies, intracranial hemorrhages occur most easily as a result of the weakness of their vascular walls.
When brain damage is localized in the area of structures that provide the speech-motor mechanism of speech, predominant disturbances in its sound-pronunciation side—dysarthria—occur.
In the etiology of speech disorders in children, immunological incompatibility of the blood of mother and fetus (for Rh factor, ABO system and other erythrocyte antigens) may play a certain role. Rhesus or group antibodies, penetrating the placenta, cause the breakdown of fetal red blood cells. As a result, a substance toxic to the central nervous system, indirect bilirubin, is released from red blood cells. Under its influence, the subcortical parts of the brain and auditory nuclei are affected, which leads to specific disturbances in the sound-pronunciation aspect of speech in combination with hearing impairment.
With intrauterine brain lesions, severe speech disorders are observed , usually combined with other polymorphic developmental defects (hearing, vision, musculoskeletal system, intelligence). They can be observed when a pregnant woman gets sick with rubella, cytomegaly, toxoplasmosis and other viral infections. Moreover, the severity of speech disorders and other developmental defects largely depends on the time of brain damage in the prenatal period. The most severe damage is observed in the first trimester of pregnancy, as well as during the entire period of embryogenesis, i.e. from 4 weeks to 4 months of pregnancy.
Pathological effects in the late stages of pregnancy usually do not cause severe malformations, but lead to a delay in the maturation of the nervous system and to disruption of the myelination of its structures.
In children with anomalies and malformations of the brain, multiple, so-called dysembryogenetic stigmas are often observed in the form of asymmetry of the skull, anomalies of the palate (high “Gothic” palate, flattened palate, bifurcated lip), developmental defects of the upper jaw, aplasia of the lower jaw, micrognathia, prognathia and etc. An example of speech disorders that arise under the influence of adverse factors on the developing fetus can be open rhinolalia, which occurs as a result of a congenital cleft palate.
Infectious and somatic diseases of the mother during pregnancy can lead to disturbances in the uteroplacental circulation, nutritional disorders and oxygen starvation of the fetus. If chronic oxygen starvation of the fetus is not severely expressed, it may not disrupt, but rather slow down the rate of fetal maturation. As a result, during a full-term pregnancy, the child is born immature, with a weakened nervous system, the processes of myelination of the nervous system are slowed down, the differentiation of nerve cells and their axons is impaired, and the formation of interneuronal connections in the brain is difficult. These factors also influence the formation of speech activity.
Disorders of intrauterine development of the fetus - embryopathies - can occur in connection with viral diseases, taking medications, ionizing radiation, vibration, alcoholism and smoking during pregnancy. The adverse effects of alcohol and nicotine on offspring have been noted for a long time.
Recently, the clinical picture of oligophrenia of alcoholic-embryopathic origin, combined with speech disorders, has been studied, and the influence of chronic alcoholism on the occurrence of various speech defects has been shown. An alcoholic embryopathic syndrome has been described, including retardation of physical, speech and mental development, and craniofacial deformities.
In alcoholic embryopathic syndrome, mild hearing impairment is noted, which also adversely affects the child’s speech development.
With parental alcoholism, there is a higher incidence of fetal death in the prenatal and perinatal periods, prematurity, intrauterine and intrapartum asphyxia, as well as higher morbidity and mortality of children in the first years of life.
In the preschool and school periods, these children attract attention with general physical weakness, mental retardation with manifestations of general speech underdevelopment, motor disinhibition, and disturbances in active attention, visual and auditory perception. Their increased distractibility is combined with low cognitive activity, personal immaturity, and learning difficulties. Currently, many works are devoted to the adverse effects of smoking on a woman’s reproductive function, as well as on the course of pregnancy and childbirth. The connection between smoking and prematurity and retardation of children in physical and mental development has been shown.
A combination of a number of unfavorable factors acting during the period of fetal development (a combination of alcoholism and smoking with toxicosis of pregnancy, with various chronic and acute viral diseases of the mother, etc.) has a particularly harmful effect on the development of the fetus.
Toxicoses of pregnancy, prematurity, short-term asphyxia during childbirth cause mildly expressed minimal organic brain damage (children with minimal cerebral dysfunction - MMD). They are characterized by lack of attention, memory, motor disorders, disinhibition, and various speech disorders.
Currently, in cases of mild brain failure, a special type of mental dysontogenesis is distinguished, which is based on superior age-related immaturity of individual higher cortical functions. It causes a peculiar lag in the development of speech and uneven mental development, which determine the specific learning difficulties of these children.
With minimal brain dysfunction, there is a delay in the rate of development of functional brain systems that require integrative activity for their implementation: speech, behavior, attention, memory, spatio-temporal representations and other higher mental functions.
Children with minimal brain dysfunction are at risk for developing speech disorders. Their timely identification and early stimulation of mental development can significantly improve the speech and mental prognosis of this category of children. A speech therapist and a speech pathologist need to know the early manifestations of minimal brain dysfunction syndrome.
The main manifestations of this syndrome in the first year of life are the so-called “minor neurological signs”: in infants, these are mild disturbances of muscle tone, which usually do not interfere with active movements, but are persistent; mildly expressed involuntary movements in the form of tremors, general shudders; delayed sensorimotor development (especially hand-eye coordination); lag in the development of fine differentiated movements of the fingers, the formation of object-manipulative activity; delay in preverbal and initial verbal development. All these signs are combined with mild neurological symptoms.
Speech disorders occur more often in males. Recent studies have shown differences in the development of the right and left (speech) hemispheres (hemispheres) depending on gender. The left hemisphere primarily performs speech function, and the right hemisphere primarily performs visual-spatial gnosis. Boys develop their right hemisphere faster than girls. In girls, on the contrary, the left hemisphere develops faster, and therefore they have earlier periods of speech development. In addition, girls develop more pronounced interhemispheric interaction earlier, which contributes to better compensation for brain damage.
In addition, the reason that determines the predominance of speech disorders in males may be intellectual and speech disorders associated with specific changes in the structure of the X chromosome.
Early organic brain lesions, combined with unfavorable conditions of upbringing and the child’s environment in the first years of life, play an important role in the occurrence of speech disorders in children.
Emotional deprivation (lack of emotionally positive contact with an adult) is of great importance.
Particular attention is paid to disruptions in the relationship between mother and child in the first years of life. It is known that normal preverbal development in the first year of life, which is important for the formation of speech function, is possible only with adequate interaction between the child and his mother or another person close to him.
Speech disorders can also arise as a result of the influence of various unfavorable factors on the child’s brain and at subsequent stages of its development. The structure of these speech disorders varies depending on the time of exposure to harmfulness and the location of brain damage.
When the immature brain is damaged, there is no complete correlation between the location, severity of the damage and long-term consequences in terms of speech disorders. Already almost a hundred years ago, it was shown and then confirmed by subsequent studies that congenital or early acquired damage to the left hemisphere in children does not so often lead to cortical speech disorders (alalic or aphasic in nature, depending on whether the damage occurs in the prelinguistic period or during the period already formed speech), as is the case with similar damage in adults. It is known that skull injuries in a child with developed speech are much less likely to cause aphasia than in an adult. Brain plasticity is largely determined by the immaturity of brain structures. This explains the lack of a clear correlation between the severity and location of a child’s brain damage and the incidence of speech disorders. There are indications in the literature that even complete removal of the left hemisphere in a young child may not cause specific speech disorders. This is explained by the plasticity of the child's brain and the more diffuse presence of speech zones in the child's immature brain, which are represented more widely in both hemispheres. There is an inverse relationship between the plasticity of the nervous system and the degree of myelination of neurons: the less myelination, that is, the less their maturity, the greater their plasticity.
This is manifested in the fact that the axon of a nerve cell, which cannot form a synapse (a special formation that communicates between nerve cells) on its damaged side, can form it in a healthy hemisphere. But this is only possible if the myelination of the cortical parts of the brain is not yet complete and not all synaptic formations in the healthy hemisphere have already been formed.
Unilateral damage to the cerebral cortex in a young child leads to qualitatively different disorders than in adults. If in adults aphasia usually occurs with damage to the dominant left hemisphere, then in children they more often occur with bihemispheric damage; in addition, even damage to the right (usually subdominant) hemisphere can cause significant disturbances in speech development.
Thus, when assessing the role of an exogenous-organic factor in the occurrence of speech disorders in childhood, it is necessary to take into account: the time, nature and localization of damage, features of the plasticity of the child’s nervous system, as well as the degree of formation of speech function at the time of brain damage.
Hereditary factors also play a certain role in the etiology of speech disorders in children. Often they are predisposing conditions that develop into speech pathology under the influence of even minor adverse influences.
In some cases, hereditary factors act as leading causes. For example, the literature provides data that rhinolalia caused by cleft palate in 10-30% of cases can be associated with hereditary factors (P. G. Svetlov, 1962; A. Ya. Piskunov, 1960, etc.) . According to A.E. Gutsman (1980), the frequency of hereditary forms of rhinolalia is only 1.31%.
According to S. A. Gridnev (1976), hereditary burden among people who stutter is 17.5%. The role of hereditary factors in the occurrence of written speech disorders (dysgraphia, dyslexia) is noted.
Hereditary factors in the occurrence of speech disorders usually act in combination with exogenous-organic and social ones. They can also play a leading role in the occurrence of certain types of speech disorders, combined with general changes in the nervous system. These are speech disorders observed in chromosomal syndromes and hereditary degenerative diseases of the nervous system, which constitute a special group of so-called secondary speech disorders. Their features are determined by the disease itself.
Chromosomal syndromes (or chromosomal diseases) are congenital and usually do not have a progressive course. With almost all chromosomal syndromes, there is a lag in the physical and neuropsychic development of the child, and speech development is also impaired to one degree or another.
Chromosomal syndromes are divided into two groups: syndromes associated with changes in the number or structure of autosomes, and syndromes caused by changes in sex chromosomes. The most pronounced disturbances of speech development and speech disorders are observed in the first group of syndromes. They are usually combined with intellectual disability, severe defects and developmental anomalies. An example would be speech impairments in Down syndrome, which are detected in late manifestations by significant underdevelopment of speech.
In recent years, special attention throughout the world has been attracted to the problems of speech disorders in children with specific changes in the structure of the X chromosome (fragile or fragile X chromosome syndrome), which are usually combined with manifestations of varying degrees of mental retardation, observed mainly in boys. Speech disorders in this syndrome are polymorphic: general speech underdevelopment, dysarthria, and sometimes stuttering. An accelerated rate of speech, combined with perseverations, is considered characteristic; as well as motor disinhibition and affective disorders.
Hereditary degenerative diseases of the nervous system are caused by changes in genetic information. They are based on gene mutations leading to disruption of the synthesis of certain structural proteins or enzymes, which causes various disorders.
Speech disorder syndromes are observed in many hereditary metabolic diseases. The first sign of impaired neuropsychic development of a child is often various speech disorders.
Specific speech disorders are also observed in phenylketonuria , a hereditary disease caused by impaired phenylalanine metabolism, and other hereditary metabolic diseases. All these speech disorders are considered as syndromes in the structure of hereditary metabolic diseases of the nervous system. Early nutritional therapy can significantly prevent the severe course of the disease, subsequent decline in intelligence and underdevelopment of speech.
It is important for a speech therapist to remember the possibility of such diseases, the need for their early diagnosis and treatment; it is advisable to refer children with suspicions of this pathology to medical genetic consultation.
So, the etiological factors causing speech disorders are complex and polymorphic. The most common combination of hereditary predisposition, unfavorable environment and damage or disruption of brain maturation under the influence of various unfavorable factors.
Analysis of the etiology of speech disorders helps distinguish “primary” speech disorders associated with damage or dysfunction of speech mechanisms from “secondary” ones observed in children with intellectual disabilities or sensory defects, as well as in various ongoing diseases of the central nervous system.
Conclusions and problems
The basis for studying the etiology of speech disorders is the evolutionary-dynamic approach and the principle of dialectical unity of the biological and social in the development of speech.
Social factors (functional forms of speech disorders) play a major role in speech development disorders and in the occurrence of neurotic speech disorders. The social environment surrounding the child is not only a condition, but also a source of speech development.
The material substrate of the speech function is the nervous system. Therefore, when the nervous system is damaged and its maturation is impaired under the influence of various factors, various speech disorders (organic central forms of speech disorders) are most often observed. Many types of speech disorders arise under the influence of various unfavorable factors affecting the developing brain of a child. Various somatic and metabolic diseases can be both favorable conditions for the occurrence of speech disorders, and in some cases their direct causes. Important questions about the etiology of speech disorders are:
• study of the causes of systemic speech disorders of cortical origin (alalia, aphasia) taking into account the location, nature and time of brain damage;
• determination of the role of hereditary factors in the occurrence of various types of speech disorders;
• detailed study of the causes and predisposing conditions to the occurrence of various forms of stuttering;
• study of statistical information on the spread of speech disorders and their causes.
Speech disorders (psychological classification)
To determine how much the defect can be influenced and corrected, a psychological and pedagogical classification was invented. Correction occurs during speech therapy sessions.
Deviations from the point of view of psychology and pedagogy are:
- Phonetic-phonemic - the child pronounces phonemes incorrectly because he also perceives them incorrectly.
- General speech underdevelopment - there are problems with all components of the articular system. The child develops speech late, it is poor, and it is difficult for him to pronounce some sounds.
- Stuttering – communication means are developed correctly, the problem is only in their use.
According to this classification, children can be divided into 3 conditional groups:
- They don’t pronounce individual sounds, there are no other problems.
- There are problems in the perception of sounds and their reproduction. Children do not distinguish some sounds, do not see articulatory and acoustic differences. They rearrange syllables when speaking, write and read poorly, and “swallow” the endings of words.
- They have general speech underdevelopment. They do not put sounds into syllables, have a small vocabulary, and do not speak coherently. If a speech therapist does not begin to treat such children on time, they may have huge communication problems.
Speech disorders affect the mental functions of a preschooler. The attention of such children is often characterized by instability. They have difficulty generalizing, comparing and analyzing, and perceiving verbal instructions. Such children are characterized by poor coordination, they are slow and awkward, and have underdeveloped fine motor skills. A child with severe disabilities lacks self-confidence, is touchy, and has difficulty establishing contacts.
Prevention of speech disorders: what should be done?
Speech problems vary and can develop at any stage of a child’s development. In many cases they can be averted. For example, from the first days of life it is imperative to communicate with a newborn. And, to the best of your ability, give communication different emotional shades (rejoice, surprise, worry, etc.).
Speech is a complex mental process. The baby will begin to talk when the brain, hearing and articulatory apparatus have reached a suitable level of development. This depends largely on the environment and health status. The child must develop, communicate and receive vivid emotions, otherwise he may develop physical and mental delays.
Sometimes communication with loved ones for younger preschoolers is limited only to monotonous everyday situations. It is not surprising if speech disorders arise against this background.
The tips of human fingers contain nerve endings connected to different parts of the cerebral cortex, including speech. It is very important to perform finger exercises and massage the fingertips in the form of a game. This develops both speech and memory. During the development of the child, it is also necessary to pay attention to finger motor skills: organize games with construction sets, plasticine, give lacing and busy boards.
Ways to correct and prevent speech errors
How to prevent speech errors? Work on your speech should include:
- Reading fiction.
- Visiting theaters, museums, exhibitions.
- Communication with educated people.
- Constant work to improve speech culture.
Online course “Russian language”
Speech errors are one of the most problematic topics that receive little attention in school. There are not so many topics in the Russian language in which people most often make mistakes - about 20. We decided to devote the course “Russian Language” to these topics. During the classes, you will have the opportunity to practice competent writing skills using a special system of multiple distributed repetitions of material through simple exercises and special memorization techniques.
How to deal with “unruly” tongue?
Often a child does not pronounce all sounds due to the fact that his articulatory apparatus is simply not mature. You can do corrective games and exercises at home or with a speech therapist, gymnastics for the tongue and fingers, and breathing exercises. By the way, whistles and soap bubbles are not just fun, they also help develop articulation.
There are various exercises for pronouncing whistling, hissing sounds, and the letter “r”. You must first try them yourself and make sure that the child sees the articulation of an adult - how exactly this or that phoneme is pronounced.
If a child is unable to pronounce a sound, he often comes up with a simpler substitute. And the adults begin to lisp along with him. There is no way to do this. “Incorrect” words and sounds are remembered for a long time, and it is very difficult to eradicate them later. The most important stage in the development of speaking is preschool, namely 3-6 years. You should talk to your child at this time:
- no baby talk;
- clearly, in order and legibly;
- short simple sentences;
- periodically repeating new words so that the little person remembers them;
- with different intonation and tempo, emotionally.
Corrective work with a speech therapist
By the age of 6-7 years, a child should correctly pronounce sounds, operate with a rich vocabulary (consisting of different parts of speech), construct consistent sentences (gender, number, cases), conduct dialogues and monologues. If there are any persistent disorders at 4 years old, it is better to consult a speech therapist.
If your child has impaired pronunciation (motor alalia, dysarthria or dyslalia is observed), you need to teach him to control the organs of articulation. This is really a lot of work for a child, because the central nervous system, brain and peripheral nervous system are involved. Sound pronunciation is corrected in 4 stages:
- Preparatory – the ability to hear sound correctly.
- Sound production is the skills of correct pronunciation of a single sound through articulation exercises.
- Automation - honing pronunciation, introducing sound into syllables.
- Differentiation – consolidation of auditory and articulatory skills.
In the main groups of kindergartens classes are conducted with speech therapists. There are speech therapy kindergartens for children, where increased attention is paid to the development of the articulation apparatus. Speech therapy sessions are even more necessary if a serious pathology is detected. There is a special adapted preschool program for children with severe speech impairments.