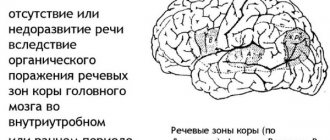
When the nervous system is damaged, the connection between the speech apparatus and the central nervous system is disrupted. Dysarthria develops, the mobility of the vocal organs - tongue, palate, lips - is limited, and articulation slows down. In children, dysarthria is accompanied by underdevelopment of speech, impaired reading and writing ability, and incorrect pronunciation of words. Dysarthria occurs as a consequence of damage to the central nervous system due to cerebral palsy, tumors, neuroinfections, injuries and other diseases. In adults, speech disorder can occur after a stroke, with the development of a brain tumor, with multiple sclerosis, Parkinson's disease, neurosyphilis and other diseases.
The neurological department of the Yusupov Hospital diagnoses and treats various diseases of the nervous system, including demyelizing diseases, Alzheimer's disease, Parkinson's disease, cerebrovascular accidents and other lesions of the nervous system. The rehabilitation center uses modern techniques to restore speech and lost abilities of the patient. To restore brain activity when the nervous system is damaged, physical therapy, exercises on simulators, and classes with a speech therapist are used. Various methods of treatment and rehabilitation are used depending on the age, condition of the patient, and the degree of damage to the central nervous system.
Making the sound "s"
The sound “s” in dysarthria is practiced depending on the complexity of the patient’s speech disorder. In difficult cases, when the patient has impaired hearing and speech, the production of the sound “s” can be done in several ways, with preliminary practice of the sounds “f”, “fa”. The speech therapist teaches the patient how to hold the tongue correctly when exhaling and at the same time pronounce a sound. When making a sound, a special thin blade is used, which is used to lightly press the tongue while exhaling and practicing the sound. This is how you can produce whistling sounds for dysarthria (anterior lingual teeth, fricative “z” and “s”). Whistling sounds are formed by a stream of air passing through the organs of speech and resembling a whistle.
When whistling sounds are produced, the air stream passes through a narrow gap that forms between the front of the tongue and the hard palate. The reference sound for the production of “s” is the sound “i”. Therefore, classes include pronunciation of the sound “i”. The doctor suggests hiding your tongue behind your teeth and smiling broadly to say “i-i-i.” Then the doctor and the patient pronounce words containing the sound “and”, the speech therapist uses various exercises. The production of the sound “s” begins after carrying out exercises with the sound “i” in various ways. Having clenched your teeth and smiling, you should silently say the sound “and”, then imagine that you are blowing on the ball. The lips should not close; the tip of the tongue should be behind the lower teeth. During the exercise, the sound “s” is heard.
The second method is performed with the help of a mechanical assistant. The tip of the tongue is located behind the lower teeth, the teeth are exposed in a smile, a thin stick is placed on the tip of the tongue, lightly pressing the tongue. The stick forms a groove in the center of the tongue. The doctor invites the patient to blow on the tip of the tongue with a strong air stream. The sound "s" is heard. In order for the exercise to be successful, you should bring the back of your hand to your mouth and watch the air stream - it should be cool and narrow. When the patient begins to pronounce the sound well, they move on to automating the sound in sentences and words.
Consultation “Methods of correction of dysarthria in modern theory and practice of speech therapy”
Alesya Samokhina
Consultation “Methods of correction of dysarthria in modern theory and practice of speech therapy”
Speech therapy work with children suffering from dysarthria is based on knowledge of the structure of speech defects in various forms of dysarthria , mechanisms of violation of general and speech motor skills, and taking into account personal qualities.
Positive results of speech therapy work are achieved subject to the following principles: gradual interconnected formation of all components of speech; systematic approach to the analysis of speech defects; regulation of mental activity of children through the development of communicative and generalizing functions of speech.
In the process of systematic and, in most cases, long-term training, a gradual normalization of the motor skills of the articulatory apparatus is carried out, the development of articulatory movements, the formation of the ability to voluntarily switch the movable organs of articulation from one movement to another at a given pace, to overcome monotony and disturbances in the tempo of speech; full development of phonemic perception.
Questions about the methodology of speech therapy with children suffering from dysarthria were developed by A. G. Ippolitova, O. V. Pravdina, M. V. Ippolitova, E. M. Mastyukova, G. V. Chirkina, I. I. Panchenko and others. Let’s consider the most used system of correctional work E. M. Mastyukova and modern methods proposed by L. V. Lopatina.
E. M. Mastyukova determines the close relationship between the development of speech, sensory functions, motor skills and intelligence; determines the need for correction of speech impairments in dysarthria in children in combination with stimulation of the development of all its aspects, sensory and mental functions, thereby achieving the formation of speech as an integral mental activity.
The success of speech therapy classes largely depends on their early start and systematic implementation.
Work on sound pronunciation is based on the following provisions:
- dependence on the form of dysarthria , level of speech development and age of the child;
- development of speech communication - the formation of sound pronunciation should be aimed at the development of communications, school and social adaptation of the child;
- development of motivation - the desire to overcome existing violations, the development of self-awareness, self-confidence;
— development of differentiated auditory attention and sound analysis;
- strengthening the perception of articulatory patterns and movements through the development of visual-kinesthetic sensations;
- step-by-step - start with those sounds whose articulation is more intact in the child. Sometimes sounds are chosen on the basis of simpler motor coordination, but always taking into account the structure of the articulatory defect as a whole; first of all, they work on the sounds of early ontogenesis;
— in case of severe disorders, when speech is completely incomprehensible to others, work begins with isolated sounds and syllables . If the child’s speech is relatively clear, and in individual words he can pronounce defective sounds correctly, work begins with these “key” sounds.
words In all cases, automation of sounds is necessary in all contexts and in various speech situations;
— in children with damage to the central nervous system, it is important to prevent severe disorders of sound pronunciation through systematic speech therapy work in the pre-speech period.
Speech therapy work for dysarthria is carried out in stages.
The first stage is preparatory, its main tasks are:
— preparation of the articulatory apparatus and formation of articulatory structures;
— nurturing the need for verbal communication;
— development and refinement of passive vocabulary;
- development of sensory functions, especially phonemic perception and rhythm reproduction.
Methods and methods of work at this stage are differentiated depending on the level of speech development. In the absence of verbal means of communication, initial vocal reactions are stimulated in the child and induce onomatopoeia, which is given a character of communicative significance.
Speech therapy work is carried out against the background of medication, physiotherapy, physical therapy and massage.
The second stage is the formation of primary communicative pronunciation skills. Its main goal is the development of speech communication and sound analysis.
Corrective work at this stage is carried out in the following areas:
1. Normalization of the innervation of the articulatory apparatus.
2. Fight against salivation.
3. Developing control over mouth position.
4. Development of articulatory movements and voice.
5. Correction of speech breathing.
6. Development of sensations of articulatory movements and articulatory praxis .
Normalization of the innervation of the articulatory apparatus is carried out using massage. Work on relaxing the muscles of the articulatory apparatus begins with general muscle relaxation, relaxation of the cervical, chest muscles, and facial muscles. A relaxing massage is carried out in doses.
Developing control over mouth position.
Lack of control over mouth position in children with dysarthria significantly complicates the development of voluntary articulatory movements.
The first stage of work is exercises for the lips, helping to relax them and enhance tactile sensations in combination with passive closing of the child’s mouth.
At the second stage, the mouth is closed in a passive-active way. At first, it is easier for a child to close his mouth when his head is tilted, and easier to open when his head is slightly tilted back.
At the third stage, active opening and closing of the mouth is trained according to verbal instructions.
Articulation gymnastics.
At the initial stages, work is carried out with the maximum connection of other, more secure analyzers. Articulatory gymnastics is differentiated depending on the form of dysarthria and the severity of damage to the articulatory apparatus. The development of articulatory motor skills is carried out systematically, over a long period of time, using a general complex and specific exercises.
Voice development.
For the development and correction of voice in dysarthric children, various orthophonic exercises are used, aimed at developing the coordinated activity of breathing, phonation and articulation. of great importance for correction .
Correction of speech breathing.
Breathing exercises begin with general breathing exercises. The goal is to increase breathing volume and normalize its rhythm. Breathing exercises are carried out before meals, in a well-ventilated area. The child is taught to breathe with his mouth closed, and exercises are carried out to train nasal exhalation.
Development of sensations of articulatory movements and articulatory praxis .
For the development of articulatory praxis, early therapy work , expansion and enrichment of the child’s speech experience, as well as the predominance of special speech exercises over purely articulatory ones are of great importance.
Correction of sound pronunciation.
The principle of an individual approach is used. The method of sound production and correction is selected individually. If the pronunciation of several sounds is impaired, consistency in work is important. Before calling and staging sounds, it is important to distinguish them by ear. By modeling this or that articulatory structure for the child, the speech therapist stimulates the evocation of an isolated sound, then automates it in syllables, words and in contextual speech.
There are several techniques for producing sounds for dysarthria . The most common method the so-called phonemic localization. The main methods of work are : motor-kinesthetic and auditory-visual-kinesthetic.
When developing sound pronunciation skills, a speech therapist works to automate and differentiate sounds and develop pronunciation skills in various communication situations. Sounds are fixed in words and sentences.
For automation, the technique of simultaneous pronunciation of a sound and the image of its symbol is used - writing and speaking.
For children who cannot write, the sound is made at the same time as finger tapping or foot tapping. The new sound is then fixed in various syllables. Gradually move from simple exercises to more complex ones, speeding up the pace of exercises.
When working on sound, it is important to identify the child’s intact compensatory capabilities.
Correction of the sound pronunciation aspect of speech is combined with work on its expressiveness.
The work is carried out by imitation. The content and methods of work vary depending on the nature and severity of dysarthria , and the general level of speech development.
In all cases, the main task of speech therapy work for dysarthria is the development and facilitation of speech communication, and not just the formation of the correct pronunciation of sounds.
Lopatina L.V., in the process of speech therapy work to overcome phonetic-phonemic disorders in preschoolers with erased dysarthria , determines the following tasks:
-formation of psychophysiological mechanisms that ensure mastery of the phonetic side of speech (sensory and motor parts of the speech process)
;
- formation of speech skills of phonetically correct speech, intonation expressiveness.
In the process of speech therapy work, the implementation of these tasks is carried out in their unity and interconnection.
The system for overcoming phonetic-phonemic disorders includes the following sections:
1. development of manual motor skills and motor skills of the articulatory apparatus;
2. formation of correct articulation of sounds and automaticity of their pronunciation in various phonetic conditions;
3. formation of intonation expressiveness of speech;
4. formation of perception of oral speech.
I. Development of manual motor skills and motor skills of the articulatory apparatus.
Work within this area is based on the following provisions:
-level organization of movements, which allows one to decompose a complex motor act into its component components and identify the state of the cerebral levels, their role in the regulation of movements and action;
- the relationship between fine differentiated motor skills of the hands and articulatory motor skills. With normal development, the child masters the sound side of speech simultaneously with the development of general motor skills and differentiated hand movements. Systematic exercises that train finger movements, along with a stimulating effect on speech development, are a powerful means of increasing the performance of the cerebral cortex;
- complex interaction of the kinesthetic and kinetic basis of movements. To carry out a motor act, the presence of two components is necessary: a kinesthetic basis, which provides a differentiated composition of complex movements, and a kinetic structure, which underlies the formation of smooth motor skills that occur over time (A. R. Luria)
. The kinetic program is ensured by the participation of its brain mechanism for creating a kinesthetic scheme of voluntary movement;
- provisions on the role of kinesthesia in movement control. Voluntary movements and actions require constant comparison of the planned act with the one actually reproduced. Continuous feedback signals must be received from the movement being performed, constituting the content of reverse differentiation and constantly being compared with the planned action.
Work on the development of manual and articulatory motor skills is carried out in two directions.
1. Formation of the kinesthetic basis of movement.
The main objectives of this area of speech therapy work are :
-organization of motor impulses directed to certain muscle groups and clarification of the composition of the motor act;
-development of kinesthetic analysis and synthesis of kinesthetic afferentations of manual and articulatory movements.
In the process of forming the kinesthetic basis of hand movements, the hands and fingers are given various positions, which the child reproduces with his eyes closed (or behind the screen)
. When forming the kinesthetic basis of articulatory movements for the development of motor-kinesthetic feedback, special exercises are carried out aimed at clarifying the position of the articulatory organs during the pronunciation of correctly pronounced sounds. When performing them, children's attention is constantly drawn to the kinesthetic sensations that arise. Initially, these exercises are based on visual images of movement, which are then eliminated.
2. Formation of the kinetic basis of movement.
The main objectives of the second direction of speech therapy work are :
- unification, generalization of successive impulses into a single, time-organized motor stereotype, transforming individual motor skills into smooth, serially organized ones;
-development of static and dynamic coordination of movements.
In the process of forming the kinetic basis of hand movements, exercises are carried out aimed at developing a system of movements consisting of “basic”
and
“background”
components
(according to A. N. Bershtein)
or a series of similar movements that make up a single motor skill.
The development of dynamic coordination of hand movements is carried out in the process of performing both sequential and simultaneously organized movements.
In the process of forming the kinetic basis of articulatory movements, the main attention is paid to exercises aimed at developing the necessary range of movements, mobility of the organs of the articulatory apparatus, strength, accuracy of movements, and developing the ability to hold the articulatory organs in a given position.
Work on the formation of the kinesthetic and kinetic foundations of manual and articulatory movements will be carried out simultaneously.
II. Formation of correct articulation of sounds and automaticity of their pronunciation in various phonetic conditions.
After the formation of the correct articulatory pattern of sound in the process of performing articulatory exercises, the automaticity of its pronunciation in various phonetic conditions is developed. It is recommended to start implementing the automaticity of pronunciation of a newly formed sound in all variants of defective pronunciation with the structure of the syllables GS (vowel - consonant, and then SG (consonant - vowel)
. This sequence of work is due to the fact that in the structure of a syllable of the SG type, its constituent sounds, according to their articulatory-acoustic characteristics, are fused with each other in such a way that they can more fully contain all phases of articulation.
Automation of sound in combination with any vowel is carried out from syllables to words , and then to sentences in order to quickly and more naturally introduce the sound in a given syllable structure into contexts of varying complexity. After achieving automaticity in the pronunciation of a sound alternately with various vowels in the structure of a syllable of the GS type, the sound is also automated in speech material, including the structure of the SG syllable.
III. Formation of intonation expressiveness of speech.
Since the phonetic side of speech represents a close interaction of its main components (sound pronunciation and prosody)
and since children with erased
dysarthria have violations of a number of prosodic elements of speech, in the process of speech therapy , work is done to form intonational expressiveness of speech.
This work is preceded by exercises. They prepare children to perceive intonation expressiveness, contribute to its development, and create the prerequisites for mastering logical stress and correct division of phrases.
Work on rhythm is carried out in two directions: perception and reproduction of various rhythmic structures.
Speech therapy work on the formation of intonation expressiveness of speech is carried out in stages.
Stage 1. Formation of ideas about intonational expressiveness in impressive speech.
The tasks of this stage include:
- show children that human speech has a variety of intonations, which is achieved by changing the pitch, strength, timbre, and modulation of the voice, that intonation gives color to speech and helps express feelings;
-introduce children to various types of intonation and means of indicating them, as well as teach them to distinguish between various intonation structures in impressive speech
In accordance with the identified tasks, work is carried out in five directions:
1) the formation of general ideas about the intonational expressiveness of speech. The speech therapist reads the same story twice. The first time without intonation of the text, the second - expressively. The speech therapist explains to children that the voice can be changed when reading, that the voice can convey questions, joy, threats, etc.
2) familiarity with narrative intonation, the means of its expression and methods of designation. The speech therapist pronounces a sentence with a narrative intonation and invites the children to determine what this sentence expresses.
3) differentiation of intonation structures of sentences in expressive speech. This work is carried out on the material of rhymes, dialogues , and fairy tales. Children must learn to imitate voices.
IV. Formation of perception of oral speech.
Speech therapy work to overcome phonemic disorders in preschoolers with erased dysarthria is carried out taking into account the following provisions:
- modern ideas about the multi-level structure of the process of speech perception (N. I. Zhinkin, I. A. Zimnyaya, E. I. Vinarskaya)
;
- provisions on the relationship between elementary and higher mental functions in the process of child development;
-scientific data on the stages of development of phonemic functions in ontogenesis.
When developing this technique, some techniques and methods described in the works of V.K. Orfinskaya, D.B. Elkonin, E.F. Sobotovich, R.I. Lalaeva were used in an adapted version.
Work to overcome phonemic disorders is carried out in stages.
Stage 1. Formation of perception of oral speech at the phonetic level.
The objectives of this stage are:
-development of speech sound recognition;
-development of the stimulating function of the speech-hearing analyzer;
-formation of auditory control over the quality of one’s own pronunciation;
-creation of favorable conditions for the subsequent formation of phonemic functions.
Work at this stage is carried out in two directions.
1) Formation of perception of oral speech in the process of imitation of syllables .
2) Formation of perception of oral speech in the process of distinguishing correctly and distortedly pronounced sounds.
- recognition of distorted pronunciation, different from one’s own, in someone else’s speech;
- recognition of distorted pronunciation similar to one’s own in someone else’s speech.
The development of auditory control is carried out simultaneously with the formation of the correct articulatory structure of sound, using visual perception of tactile and kinesthetic sensations.
Stage 2. Formation of perception of oral speech at the phonological level.
Due to the fact that clear phonemic ideas about the sound composition of the language contribute to the improvement of correct sound pronunciation, the task of this stage includes the development of the functions of the phonemic system.
The formation of phonemic functions is carried out in two directions: the development of phonemic perception (differentiation of phonemes)
and the development of phonemic analysis and synthesis.
Work at this stage begins with consistent clarification of the pronunciation and auditory images of the sound being practiced and is carried out in three directions.
1) Clarification of sound articulation based on visual, auditory, tactile perception, and kinesthetic sensations.
When clarifying the correct articulation of a sound, attention is paid to the work of the articulatory organs when pronouncing it. To consolidate the visual image of sound, children are offered symbolic images.
2) Isolation of sound against the background of a syllable.
Children are offered a number of syllables from which they need to select a given sound. Syllables should not contain oppositional sounds.
3) Isolation of sound against the background of a word.
This work is carried out on the material of words containing this sound and not having it. Words with similar acoustic sounds and sounds that are mixed in pronunciation are excluded.
Thus, dysarthria requires early , long-term and systematic speech therapy work . Its success largely depends on the relationship in the work of a speech therapist and a neurologist or neuropsychiatrist, a speech therapist and parents , and in case of obvious motor disorders - a speech therapist and a massage therapist , a specialist in physical therapy.
Setting the sound “d”, sound “t” and “t”
Stating the sound “t” for dysarthria and “d” begins with exercises for the tongue, which help increase its flexibility and relieve tone. The patient raises the tongue up, touching the tip of the tongue to the palate, the tongue is directed to the right, to the left, and speech therapy gymnastics is performed. Then the doctor suggests tapping with a hammer (tongue). The patient makes the sound “t” by raising the tongue to the palate and moving it forward between the front teeth. A soft consonant is produced by raising the tongue closer to the roof of the mouth, creating a narrower passage for air to escape than a hard consonant.
The production of the sound “th” for dysarthria is carried out using the method of pronunciation of a soft consonant sound. A speech therapist works with the patient on the pronunciation of soft and hard consonant sounds. Using a spatula, the doctor presses the tip of the tongue, lowers it behind the lower teeth, the child pronounces the syllable “ta” - the result is “cha”. The doctor asks the child to click his tongue. Then the child exhales while clicking, rather than inhaling air - the sound “ti” is obtained. To enhance softness, the sound “t” is pronounced between two vowels.
When pronouncing the sound “d,” the vocal folds close, the palate lowers, and vibration is felt in the larynx. The sound “d” can be produced in several ways: by imitation, from the sound “b”, from the sound “t”. From the sound “t”: the doctor places one of the child’s hands on his larynx, the other on the child’s larynx. Then he pronounces the sounds “t” and “d” in turn, asking to pay attention to the difference in the vibration of the larynx when pronouncing the sounds. Draws attention to vibration when pronouncing the sound “d”. From the sound “b”: The tip of the child’s tongue is located between the teeth. The doctor asks to pronounce the syllables “ba-ba-ba”, at the moment of pronunciation he parts the child’s lips - the syllables “da-da-da” are heard.
Making the sound "n"
Articulation and production of the sound “n” is carried out. During articulation, the lips are in a neutral position, the tip of the tongue touches the upper teeth, and vibration occurs in the nasal cavity when pronouncing a sound. Sound production is carried out using two methods: imitation and from the sound “m”. Method of imitation: the child touches his nose with a finger of one hand, and the doctor’s nose with a finger of the other hand. The doctor shows the position of the tongue in the mouth while pronouncing the sound. The child feels the vibration and tries to repeat it.
Method for the sound “m”: the child’s tongue is inserted between closed lips, the child pronounces a drawn-out “m”. A hint of the sound “n” is heard. As you get used to the interlabial pronunciation of the sound “n” in words, the lips are parted with your fingers. The tongue is then moved to its normal position towards the upper teeth.
Making the sound "l"
Incorrect pronunciation of the “l” sound or omission of the “l” sound is called lambdacism. There are several types of lambdacism:
- When pronouncing the sound “l”, the sound “u” is heard - bilabial type.
- The root part of the tongue falls on the soft palate; when pronouncing sounds, the air flow goes through the nose and changes the sound “l” to “ng”, speech becomes nasal - nasal type.
- During the pronunciation of sounds, the tip of the tongue moves into the interdental space - interdental type.
- The sound “l” is not pronounced at all.
A child may not pronounce the sound “l” for several reasons:
- The child has a short hypoglossal ligament.
- The muscle tissue of the tongue is weakened.
- The child does not perceive the sound “l”, phonemic hearing is impaired.
Preparation for producing the “l” sound for dysarthria begins with articulation. The organs of articulation – lips, palate, tongue – should be positioned correctly. The teeth should not close together, the tip of the tongue should rest against the upper gums or teeth, it should be tense. The upper palate and the root of the tongue should be raised, vibration is created in the area of the vocal folds. The production of sound depends on the type of lambdacism. With bilabial lambdacism, sound pronunciation is impaired due to incorrect positioning of the lips. In this case, use the exercise with a smile, the teeth are clenched and the lips part in a smile. The speech therapist conducts articulation gymnastics with the child, activities during which lip tension is relieved. Also, the sound “l” can be made by imitation. The speech therapist shows the child the correct position of the lips, tongue, teeth and pronounces the sound. At this time, the child’s palm is placed on the doctor’s cheek, and he feels the vibration being created. The sound “l” refers to complex sounds, the production of which is formed by the age of 6 years of a child’s life.
Articulatory motor skills
The following types of dysarthria are distinguished:
- Bulbar - caused by local paralysis of the muscles that are involved in articulation, it is accompanied by difficulties in swallowing;
- Cerebellar - occurs in the presence of a pathological process in the cerebellum, characterized by extended speech with constantly changing volume;
- Cortical - is a consequence of damage to the parts of the cerebral cortex that are responsible for the muscles involved in articulation, accompanied by incorrect pronunciation of syllables, but the general structure of the word is preserved by the child;
- Extrapyramidal (subcortical, hyperkinetic) - develops with disorders in the subcortical nodes, characterized by slurred, connected speech with a nasal tint;
- Pseudobulbar - diagnosed with central muscle paralysis, its main symptom is monotony of speech;
- The erased form is characterized by a violation of the pronunciation of hissing and whistling sounds.
With dysarthria, the motor skills of the articulatory apparatus are impaired. Slow, insufficiently precise movements of the tongue and lips appear. There is a disorder of chewing and swallowing. Pronunciation is impaired due to insufficiently clear articulatory motor skills. Speech is somewhat slow, and there is blurring when pronouncing sounds. More often, the pronunciation of sounds that are difficult to articulate suffers: zh, sh, r, ts, ch. Voiced sounds are pronounced with insufficient participation of the voice. Soft sounds are difficult to pronounce and require adding to the main articulation the raising of the middle part of the back of the tongue to the hard palate.
Some patients with dysarthria cannot puff out their cheeks, stretch out their lips, or close them tightly. The movements of the tongue are limited, the patient cannot lift the tip of the tongue up, turn it to the right, left, or hold it in this position. The soft palate is often inactive, and the voice takes on a nasal tone.
The consequence of dysfunction of the articulatory apparatus is a severe pronunciation defect. Speech becomes slurred, slurred, and quiet. Due to the inactivity of the lips and tongue, the pronunciation of vowels becomes unclear; they are pronounced with a strong nasal exhalation.
With severe dysarthria, there is deep damage to the articular muscles and complete inactivity of the speech apparatus. The patient is completely speechless. Sometimes he makes inarticulate sounds.
Making the sound “e”, “y” and other vowels
The production of the sound “y” for dysarthria, as well as the sounds “u”, “e”, “o”, “a”, “i” is carried out first. The speech therapist clarifies the articulation of vowel sounds. Then work begins with soft sonars, then with their hard sound pairs. Speech therapy massage, articulation gymnastics, and breathing exercises are performed beforehand. The doctor invites the child to take a deep breath through the nose, open his mouth slightly with a smile, and point the tip of his tongue toward the lower incisors. Exhale and whisper the sound “e”, then repeat the exercise with your voice.
Speech hearing
In order for a child to successfully learn a new pronunciation, he must distinguish it by ear. This is also important for differentiating different groups, for example, voiced and deaf.
Therefore, development begins with the use of non-speech material. For example, a child is shown how paper crumples, a pencil knocks on the table, water pours from glass to glass. Afterwards he is asked to turn away and he must determine the action by ear.
You should not give your preschooler the opportunity to guess! Any attempts to randomly give out an answer must be stopped. The speech therapist does not answer questions, but you can suggest the thought “what do you think is babbling?” or “what’s rustling?”
You can show pictures of musical instruments and show a sample of their sound. Afterwards, the passages are turned on in random order, and the child must show the correct answer.
Another simple task that can be easily done at home. The preschooler is asked to close his eyes and listen to the world around him. He must determine what is happening around him. For example, the car is driving, mom is washing dishes in the kitchen, the cat is meowing, etc.
Only after the discrimination of non-speech sounds begins to go well, do they move on to speech sounds. To begin with, use vowel sounds.
You cannot give an image of a letter - this will confuse the child and confuse him. The signs proposed by Tkachenko are used as symbols.
The preschooler is explained how to pronounce the sound “A” (with his mouth wide open) and shown a large red circle - it will be a symbol. Then the sounds “U” and “O” are analyzed. Tasks are offered to determine sound during silent articulation.
Little by little they learn to identify the place of sound. For example, they call the series “O, A, O” and ask them to say which sound is the first. To facilitate understanding, they show a picture of a train or car (telling that there is a beginning, middle and end).
Only after this stage has been perfectly mastered do they move on to producing the “C” sound in a child with dysarthria and others.
How to make the sound "r"
An experienced speech therapist knows how to make the sound “r” for dysarthria, how to make the process of automating the sound “r” interesting. Making the sound “r” with dysarthria can take a long time. After warming up, the doctor asks the child to memorize the words, then repeat them using pictures. The pictures depict objects, flowers, plants, animals whose names contain the sound “r”. Such activities train memory and correct sound pronunciation. Methods used to make the sound “r”:
- Imitation.
- Through articulation.
- Mechanical assistance: from the reference sound, from the articulatory structure.
Supporting measures
Often with dysarthria there is an increased or decreased tone of the speech organs. In order to cope with this problem, speech therapy massage is used.
It can be either manual or probe. The procedure consists of stroking and light pressure on different areas. This is often done at the beginning of each lesson. This makes the muscles susceptible to the effects.
Dysarthria is often accompanied by increased salivation. To reduce secretion, give jelly, chew biscuits and crackers. Before the lesson, the child is seated on a chair, asked to throw back his head and imitate chewing. The speech therapist can massage the points behind the ears and the junction of the jaws. This will reduce the work of the glands.
There are no uniform patterns when producing sounds. For each child, methods are selected individually.
Making the sound "th"
The sound “th” refers to the middle lingual, oral, fricative, consonant, voiced, soft sounds. Before setting the sound “th”, speech therapy gymnastics is carried out, then the sound is set by imitation, which is accompanied by tactile sensations and demonstration of articulation. Sound production can be done by pronouncing the sound combinations “ya” at a fast pace, using the sound “z”, pressing the tip of the child’s tongue when pronouncing the sound - the sound “th” is obtained. The sound “th” is heard when the sound “h” is pronounced.
Setting the sound "ts"
The sound “ts” is introduced after the child begins to pronounce the sounds “s” and “t” well. With the rapid repetition and merging of the sounds “t-s”, the sound “ts” is obtained. The sound of the sound “ts” can be achieved by imitation. The child’s palm is brought to the speech therapist’s mouth, the sound “ts” is pronounced with a strong exhalation - the child feels a stream of cold air on his palm. The doctor shows the child the position of the tongue, lips and teeth when pronouncing a sound. Then the child must repeat several times the syllables consisting of the sound combination “ts” and vowels.
When pronouncing a sound, the tip of the tongue rests on the front teeth, the tongue is curved and raised, the lateral edges of the organ are tense. When pronouncing a sound, the tip of the tongue moves away from the front teeth, increasing the flow of air. The part of the tongue adjacent to the palate is lowered. When pronouncing, the teeth are brought together, the lips are stretched into a smile. The air comes out with a push when the palate and tongue open; the palm applied to the mouth feels a strong and cold stream. To consolidate the result, the doctor pronounces tongue twisters with the child and plays games to identify the sound “ts” with his eyes closed.
In case of interdental sigmatism, for good pronunciation of the sound, a spatula or a teaspoon is used, which is used to fix the tip of the tongue on the inside of the lower teeth while pronouncing the sound. The middle part of the tongue should connect to the hard palate. With labiodental sigmatism, the lower lip interferes with the pronunciation of sounds. To ensure the purity of sound pronunciation, the doctor holds the child’s lower lip while the child learns to pronounce forward and backward syllables containing the sound “ts”. The production of the sound “ts” is carried out through daily activities with the child, through games, and pronouncing tongue twisters.
Setting the sound "sh"
Setting the sound “ch” for dysarthria and the sound “sh”, “d”, “zh”, “sch”, “ts”, “g”, “b”, “r”, as well as setting the sound “z” for dysarthria carried out in the second stage. Methods for making the sound “sh” for dysarthria are used after the child learns to make a cup with his tongue. The wide tongue rises to the upper teeth, preventing air from passing through the edges. The tip of the tongue forms a gap with the palate. The child should exhale warm air with some effort; vibration should not be created in the larynx. The sound “sh” can be corrected from the sound “r” and the syllable “ksh”. Sound production is carried out using a spatula or spatula, which helps slow down the vibration of the tongue and the result is hissing. Sound production can be done by imitation.
Stages of speech therapy work
Speech therapy work for dysarthria is carried out in stages. The main goal of the first, preparatory stage is to prepare the articulatory apparatus for the formation of articulatory patterns, correction of breathing and voice. An important task at this stage is the development of sensory functions, especially auditory perception and sound analysis, as well as the perception and reproduction of rhythm. Speech therapy work is carried out against the background of medication and physiotherapeutic treatment, massage and physical therapy.
At the second stage, primary communicative pronunciation skills are formed. Its main goal is the development of speech communication and sound analysis. The speech therapist works to correct articulation disorders. In case of spasticity, they work on relaxing the muscles of the articulatory apparatus. Control over the position of the mouth is developed, articulatory movements develop, speech breathing is corrected, the voice, sensations of articulatory movements and articulatory praxis develop.
The formation of sound pronunciation in dysarthria includes the production and consolidation of sounds in speech. The first group of sounds includes phonemes that are the easiest in terms of articulation and acoustically distant from each other. These are the sounds a, y, p, m, n, k, s, x, v, o, l, t, s. These sounds, being the simplest ones, are worked out to the norm. Along the way, these phonemes are used to develop phonemic perception and sound analysis skills (identifying sounds from a number of others, from syllables, in simple words).
Tongue twisters for dysarthria are a phonetic means of developing the mobility of the articulatory apparatus. When using tongue twisters, adhere to the following recommendations:
- The work begins with simple, short, rhyming phrases (“White sheep beat the drums”);
- The principle of selection of didactic material is observed (the tongue twister should not contain words with sounds that are poorly pronounced by the patient;
- Tongue twisters are best used in games.
An individual approach to the selection of means and methods of speech therapy work at each stage of treatment for dysarthria allows specialists at the Yusupov Hospital to achieve speech restoration in patients who were abandoned in other rehabilitation centers.
Making the sound "p"
At the first stage of treatment, the sound “p” is automated and the sound “p” is differentiated. The order of sound production depends on the degree of difficulty for pronunciation, the gradual transition from easy to pronounce to difficult to pronounce sounds. The order of sounds will depend on the similarity in articulation and acoustics. The sound “p” is labiodental, oral, plosive, stop, instantaneous, voiceless. At the moment the sound is pronounced, the lips are closed and tense, then the lips open and the air pushes out. There is a small distance between the teeth, the soft palate closes the passage to the nose, the vocal cords are open. Sound production is based on imitation, speech motor rhythms are used.
general information
The production of any sounds takes place in four stages and none of them can be skipped.
Before any work, a complete examination of the child’s speech condition is required. The speech therapist will check all sounds and note the degree of defect (replacement, distortion, etc.). Then the syllable structure is checked. To do this, the child is shown pictures whose names consist of syllables of varying complexity. For example, “mom”, “dad” and others. More difficult ones - “branches”, “sleds”, etc.
The next stage is studying the phonemic side of speech. To do this, show the preschooler different pictures and ask him to name the first, last sound, or find all the pictures for a given sound.
The next stage is an examination of vocabulary, that is, vocabulary. They are shown a group of objects and asked to classify it. For example, “this is furniture” or “this is dishes.”
At the final stage, they are asked to compose a story based on the picture. Based on the information received, the speech therapist makes a conclusion and determines the goals of correctional work.
Preschoolers must have their speech organs checked. The tone (increased or decreased), structural features, as well as the length of the hyoid ligament are noted.
The peculiarity of dysarthria is that it causes various breathing problems. Because of this, speech is poorly colored, almost devoid of emotion and expressiveness.
Staging hissing sounds
Training takes place through classes; methods for producing hissing sounds depend on the diagnosis and the level of psychomotor dysfunction. The principle of an individual approach is used; classes should develop the child emotionally and intellectually. During the production of sounds, visual, auditory and tactile analyzers are connected, motor-kinesthetic, auditory-visual-kinesthetic, and didactic methods are used. Active and passive articulatory gymnastics and massage are performed.