Aphasia is a complete loss or profound disorder of formed speech function as a result of local lesions of the speech areas of the brain. In this case, the communicative function suffers severely.
Etiology:
- rupture of cerebral aneurysms, thromboembolism caused by rheumatic heart disease;
- traumatic brain injuries;
- tumor-like formations;
- infectious diseases of the brain.
The degree of damage and the structure of speech pathology depends on:
- localization of the lesion;
- size of the lesion;
- left-handedness;
- individual characteristics of the residual preserved elements of the speech system.
Aphasia can be diagnosed in both adults and children. Children's forms of pathology differ from adults in the possibility of rapid recovery.
Childhood aphasia should be differentiated from alalia. Alalia is an underdevelopment of the entire language system, and aphasia is a systemic breakdown of already formed speech activity. Speech therapy correction for alalia is the evocation and development of speech, for aphasia it is the restoration of lost function.
Classification of aphasia
- Acoustic-gnostic or sensory (damage to Wernicke's center leads to a deep disorder of phonemic hearing and has 3 degrees of understanding of addressed speech: rough, medium, light).
- Acoustic-mnestic (occurs as a result of damage to the middle and posterior parts of the temporal region, auditory-verbal memory, auditory perception, and stability of visual object images are critically affected).
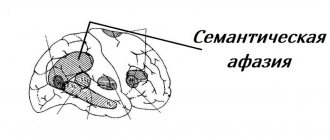
- Semantic (the defect is based on defects in simultaneous (simultaneous) capture of information, as a result, speech structures reflecting spatial categories suffer).
- Optical-mnestic (loss of relationship between the word and the image of the object).
- Afferent motor (characterized by a violation of kinesthetic sensations, nerve impulses do not regulate the correct articulation of the organs of the speech apparatus).
- Efferent motor (damage to Broca's center leads to impaired switchability between different articulatory structures).
- Dynamic (impossibility of productive independent expressive and internal speech).
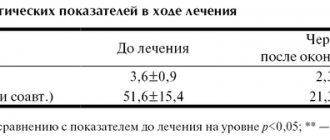
Classification of aphasia (table)
The table shows a comparison of the classification of A. R. Luria with the Boston classifications.
2.3. Classification of aphasias
Difficulties that have arisen in aphasiology (mismatch between theoretical concepts of aphasia, their classifications and clinical facts, etc.) required a new approach to the study of aphasia. A new period of development was laid by Soviet researchers. The neuropsychological study of aphasia, begun by A. R. Luria and his colleagues, made it possible to qualify the defect and establish the mechanism of the disorder underlying the speech defect. A. R. Luria created a new doctrine of aphasia, which was based on the idea of aphasia as a systemic speech disorder that arises as a result of the loss of any one factor (kinetic or kinesthetic analysis of sounds, phonemic hearing, spatial concepts, etc.) and leading each time to a specific syndrome (symptom complex), characteristic of one or another form of aphasia. This “factorial” approach, developed by A. R. Luria, was the basis for his classification of aphasias, which is fundamentally different from the classical classification of aphasias and modern foreign ones. This approach to aphasia is essential to the effectiveness of remedial training.
A. R. Luria’s identification of different forms of aphasia was based on the “principle of analysis of topically limited brain lesions,” on the one hand, and “the identification of those factors that underlie the entire complex of disorders that occur with local brain lesions,” on the other . Since the psychophysiological basis of speech is the joint activity of various analyzers and the interaction of various levels of the nervous system, it is natural that the loss of various links (or factors) from the structure of speech will be accompanied by various forms of its disorders, i.e. various forms of aphasia. All forms of aphasia differ significantly from each other in the underlying mechanism, in the clinical picture and in the psychological structure of the speech disorder. Common to all forms of aphasia is a systemic disorder of speech, and not an isolated loss of any aspect of it. Each form of aphasia occurs when a certain area of the cortex of the left hemisphere of the brain, the so-called “speech zone,” is damaged, and depends on the location of the lesion and the factor.
The classification of aphasias developed by A. R. Luria differs from the classical Wernicke-Lichtheim and modern foreign ones (“fluent” and “non-fluent” aphasias - fluent and nonfluent aphasia (Howes, 1964; Venson, \967; Goodglass, 1968); disconnection syndroms {Goodglass, Benson, etc.), expressive and receptive aphasia {Lhermitte et al.)), firstly, by the fact that the main principle of identifying the form of aphasia is the principle of isolating the mechanism (factor) underlying the violation of the functional system that provides speech . Secondly, syndromic analysis of the disorder replaced a simple description of the external picture of the disorder. Let us turn to the description of the classification of aphasia created by A. R. Luria. He studied and described seven forms of aphasia:
- efferent motor aphasia (damage to the posterior frontal parts of the cerebral cortex - 44th field, or Broca's area);
— afferent motor aphasia (damage to the posterior postcentral sections of the motor analyzer, lower parietal sections);
- dynamic aphasia (brain areas located anterior to Broca’s area and additional speech “Penfield area”);
- sensory aphasia (damage to the posterior third of the superior temporal gyrus - 22nd area, Wernicke's area);
- acoustic-mnestic aphasia (damage to the middle temporal gyrus - 21st and 37th fields);
— semantic aphasia (damage to the parietal-temporal-retro-occipital region);
- amnestic aphasia (posterior temporal and parieto-occipital areas of the cortex of the left hemisphere of the brain).
In recent years of our experimental and practical work with patients with aphasia, we have made an attempt to approach the classification of aphasia based on a new principle for considering and understanding aphasia. The experimental material we obtained together with A. A. Tsyganok (1973), and later in our theoretical-experimental work (1998,2002), gave grounds to apply a level approach to the analysis and understanding of aphasia. Here the question was considered at what level in the structure of speech the disturbances occurred and to what level of damage they correspond. We received data indicating that dynamic, semantic and amnestic forms of aphasia, in which higher syntheses in the flow of speech are disrupted, fall into one group. Acoustic-mnestic aphasia joins them. As for their brain basis, these are also the highest levels in the structure of the cortex - tertiary fields.
The second group includes afferent and efferent motor and sensory forms of aphasia, which are a consequence of violations of lower levels in the construction of speech, levels that provide sensory perception and lower forms of motor processes. The brain basis of these forms of aphasia is a violation of secondary fields in the structure of the cerebral cortex.
brain and aphasia (continued) – Previous / Next – 2.3. classification of aphasias
Periods of recovery correction
Restorative correction involves influencing all mental processes as a whole and is carried out against the background of psychotherapeutic measures. There are 2 periods in speech therapy work.
- Acute period (first 2 months after illness). Work is underway to disinhibit oppressed speech structures and prevent fixation of agrammatisms, paraphasias, and speech emboli. The correction is based on dialogical speech according to the following scheme: reflected speech - hints of the first syllable of the answer - independent answer with the choice of several words - independent answer without taking into account the number of words - independent formulation of questions.
- Residual period (after 2 months). Anomalous connections are inhibited.
Aphasia. Definition. Aphasia as a systemic defect. Classification of aphasias (according to A.R. Luria)
Aphasia is a systemic disorder of various forms of speech activity that occurs with local damage to the left hemisphere and the immediate subcortex.
Types of aphasia (according to Luria):
1. Motor aphasia. Speech as speaking is impaired.
Efferent motor aphasia (Broca's aphasia). Lesion of field 44 – lower parts of the premotor areas of the frontal lobe. Violation of the kinetic side of speech. Rough cases: inarticulate sounds, emboli (speech stereotypes) remain in speech, which remain and are pronounced constantly (maybe a swear word). The patient hears that he is saying something wrong. He tries to express everything using emboli. Mild cases: can pronounce syllables, but cannot express themselves. Perseverations are constant repetition. Phrases in speech are an inaccessible thing. Main violation: kinetic factor (smooth switching). Inhibition and updating of what follows. For smooth speech. Correct timing of movements. Disturbances in speech automation occur. Agrammatism, loss of verbs (telegraphic style). A person realizes this. Treatment: disinhibition phase - first. Secondary impairments relate to writing, reading and even understanding speech. Articulation is normal when writing and reading. In severe cases: speech understanding is impaired due to a violation of smooth pronunciation.
Afferent motor aphasia. The lower parts of the parietal region of the brain. 40 field adjacent to 22 and 42 fields. The feedback going to the brain is disrupted. Does not feel articulation (it is impaired). The kinesthetic factor is disrupted. They cannot find the right position of their lips and tongue when naming words. Subtle articulatory movements are impaired. Substitutions of close articles (g-k-x; d-l-n) may occur: robe-hadan. Patients hear the difference and try to correct it. Severe cases: they cannot speak: neither pronounce them independently nor repeat the word. The replacement of closely related articles is also visible when writing – literal paraphasia. Speech understanding suffers secondarily. Speech understanding is often intact. Treatment: disinhibit. There are emboli. Reading suffers. Can't find articulation. “The mouth doesn’t obey.” Violation of oral praxis: inflate the left cheek, right cheek, take out the tongue, etc. These tests are not available to the patient.
2. Sensory aphasia (Wernicke's aphasia). Posterior third of the superior temporal gyrus of the left hemisphere (field 22). Perception is impaired. Phonemic hearing suffers. Rough cases: they do not understand speech addressed to them. They perceive it as inarticulate noises. They cannot speak, there is no sound analysis. Their speech is “word salad.” Alienation of the meaning of words - the image behind the given word ceases to stand. Normally, if you repeat the word for a long time. The patient replaces sounds that are similar in sound (b-p; v-d). It's the same when writing. Reading, writing, and oral arithmetic are impaired. Patients are sociable (gestures, intonation, etc.). Treatment: Slowing down the Patient is the first step. Switch to other types of Activities.
3. Acoustic-mnestic aphasia. Damage to the 2nd temporal gyrus (middle parts of the temporal cortex of the brain). 21, 37 fields. Decrease in the volume of auditory-speech memory. The patient is unable to hold even small material. The memory capacity is reduced to 2 – 3 elements. Simple short phrases The patient can understand. Mechanism: the influence of interference (some kind of interference). Increased retro- and proactive inhibition of memory traces. Retro - subsequent information pushes out the previous one. Proactive – old information fills all space. Verbal paraphasia is the replacement of words in speech. Writing and reading are preserved at a small volume. The phenomenon of alienation of the meaning of words, difficulty understanding long phrases, searching for the right word, the connection between image and word - verbal paraphasia.
4. Optical-mnestic aphasia. Damage to the inferotemporal-occipital parts of the brain at the border with the 18th and 19th fields. Violation of visual-object images, object reference. The process of identifying an object is disrupted and the nomination is difficult. It's difficult to name the item. Constant search for the right word. The phenomenon of alienation of the meaning of words, but to a lesser extent than in previous cases. Skipping nouns. Speech understanding is more secure.
5. Dynamic aphasia. Damage to the premotor zone (fields 9, 10, 46). Violation of active productive speech. The patient can repeat the phrase, but cannot formulate a statement on his own. Passive speech – monosyllabic answers to questions, often echolalia (repetition of the experimenter’s last word). Essay writing method. Method of given associations. “Name some sharp objects.” Making up a story based on a picture. Mostly verbs are lost. The predicative nature of inner speech is disrupted. Speech stamps (stable expressions) are preserved.
6. Semantic aphasia. The SRW zone (37 and partially 39 fields) is the zone of intersection of the crust. The patient understands simple speech and speaks simple phrases. Spatial simultaneous perception suffers. They cannot understand logical-grammatical structures. Everything related to the spatial factor: prepositions (on, in, under, etc.). Everything related to comparison (higher-lower, easier-more difficult). Simultaneity is broken. The Patient’s logical connections are difficult to understand. Temporary structures (“Wash your hands before eating”).